
Rationale and Objectives
Most fluorine-18 fluorodeoxyglucose (FDG)-positron emission tomography with computed tomography (PET/CT) studies are performed on cancer patients. These patients are at increased risk of pulmonary embolism (PE). In this retrospective review, we determined the rate of PE, and the prevalence of associated FDG-PET findings on intravenous (IV) contrast-enhanced PET/CT.
Materials and Methods
We identified all PET/CT studies performed at our institution with a reported finding of PE between January 2005 and October 2012. The medical record was reviewed for symptoms, which were identified after the diagnosis of PE, and whether the patients received treatment. The prevalence of associated FDG-PET findings was determined.
Results
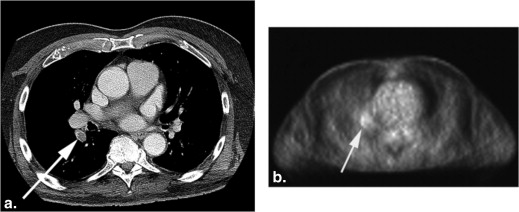
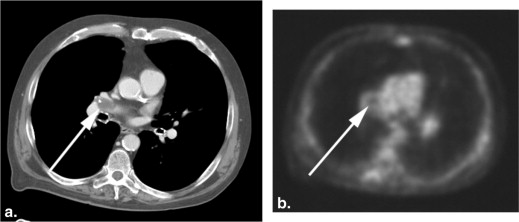
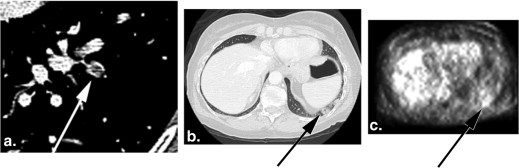
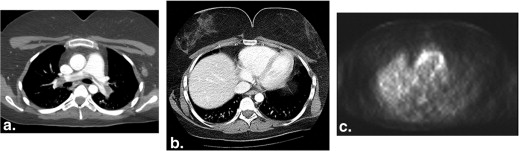
A total of 65 total cases of PE (of 182,72 total PET/CT examinations) were identified of which 59 were previously unknown. This gives an incidental PE (IPE) rate of 0.32%. Of the patients where sufficient clinical information was available, 34 of 36 (94%) were treated either with therapeutic anticoagulation or inferior vena cava filter, and 30 of 36 (83%) were asymptomatic in retrospect. Of the patients with IPE, we found nine (15.2%) with associated focal pulmonary artery hypermetabolism, three (5.1%) with hypermetabolic pulmonary infarction, and one with increased isolated right ventricular FDG uptake (1.7%). One case of chronic PE demonstrated a focal hypometabolic filling defect in a pulmonary artery on PET.
Conclusions
We found IPE in 0.32% of PET/CT scans. Focal pulmonary artery hypermetabolism or hypometabolism, and hypermetabolic pulmonary artery infarction with the “rim sign” were uncommonly associated with PE. These findings could raise the possibility of IPE in non-IV contrast-enhanced PET/CT studies.
Acute pulmonary embolism (PE) represents a potential life threatening complication of venous thrombosis and is notoriously variable in presentation. Oncology patients have a higher risk of PE and often present without the typical clinical manifestations . These so-called asymptomatic PEs are clinically significant in oncology patients. They serve as a marker for future symptomatic venous thromboembolism (VTE), a term that encompasses both deep venous thrombosis (DVT) and PE , and are associated with decreased survival . The current consensus is for therapeutic intervention in these patients despite the absence of symptoms .
Several previous studies have investigated the rates of incidental PE (IPE) on contrast-enhanced computed tomography (CT) studies in the oncologic population, with reported rates ranging from 0.58% to 4.0% . Since its approval by the Food and Drug Administration in 2000, fluorine-18 fluorodeoxyglucose (FDG)-positron emission tomography fused with concurrent computed tomography (PET/CT) has rapidly evolved into a cornerstone imaging modality in oncology. At our institution, approximately 95% of PET/CT studies are performed in patients with known or suspected malignancy, and the routine imaging protocol includes intravenous (IV) contrast. In general, most centers perform low-dose, noncontrast-enhanced CT as part of their routine FDG-PET/CT protocol. At our institution, there is a consensus between referring clinicians and the radiology department that patients undergoing PET/CT have a contrast-enhanced diagnostic quality CT unless there is a contraindication such as renal failure or contrast allergy. One previous study found IPE in 13 of 2216 patients (0.59%) who had a contrast-enhanced PET/CT . The aim of our study was to evaluate the incidence of IPE in patients referred for FDG-PET/CT studies in a much larger cohort. An additional goal was to identify and characterize associated PET findings and their relative frequency.
Materials and methods
Patient Selection
Get Radiology Tree app to read full this article<
Scan Technique
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Imaging and Chart Review
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Total Number of Cases Reviewed
Get Radiology Tree app to read full this article<
Incidence of PE
Get Radiology Tree app to read full this article<
Table 1
Pulmonary Embolism Characteristics
Total IV contrast-enhanced PET/CT scans ∗ 18,272 Number of cases with PE 65 Number of cases of incidental PE 59 (0.32%) Number of cases with chronic PE 6 Location in pulmonary artery Main PA 9/59 (15%) Lobar PA 15/59 (25%) Segmental PA 27/59 (46%) Subsegmental PA 8/59 (14%)
IV, intravenous; PA, pulmonary artery; PE, pulmonary embolism; PET/CT, positron emission tomography with computed tomography.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Demographics of Patients with IPE
Age Mean 55.8 Standard deviation 15 Range 23–84 Malignant neoplasm ∗ 57/59 (97%) Metastases 34/51 (67%) Female 30/59 (51%) Male 29/59 (49%) Treatment † Chemotherapy 30/47 (64%) Surgery 13/47 (28%) Radiation 7/47 (15%) None 19/47 (21%)
IPE, incidental pulmonary embolism.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Characteristics of Tumors
Type # IPE Total ∗ Incidence ∗ Breast 13 2563 0.51% Melanoma 10 2839 0.35% Lymphoma 6 Lung 5 Esophageal 4 Colon 3 Anorectal 2 Ewing’s sarcoma 2 Multiple myeloma 2 Other 10 No malignancy 2
IPE, incidental pulmonary embolism.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Pulmonary Emboli Characteristics
Get Radiology Tree app to read full this article<
Clinical Symptoms and Treatment with Anticoagulation
Get Radiology Tree app to read full this article<
Review of Associated FDG-PET Findings
Get Radiology Tree app to read full this article<
Table 4
PET Findings Associated with IPE
High SUV in right ventricle 1/59 (2%) Hypermetabolic pulmonary infarction 3/59 (5%) Hypermetabolic pulmonary artery 9/59 (15%) Mean SUV 2.2 ± 0.7 Max SUV 3.2 Main PA 1/9 Lobar PA 2/9 Segmental PA 4/9 Subsegmental PA 2/9
IPE, incidental pulmonary embolism; PA, pulmonary artery; SUV, standardized uptake value.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Supplementary Data
Get Radiology Tree app to read full this article<
Supplemental Figures1–4
Get Radiology Tree app to read full this article<
References
1. den Exter P.L., Jimenez D., Kroft L.J., et. al.: Outcome of incidentally diagnosed pulmonary embolism in patients with malignancy. Curr Opin Pulm Med 2012; 18: pp. 399-405.
2. Heit J.A., Silverstein M.D., Mohr D.N., et. al.: Risk factors for deep vein thrombosis and pulmonary embolism: a population-based case-control study. Arch Intern Med 2000; 160: pp. 809-815.
3. Fulkerson W.J., Coleman R.E., Ravin C.E., et. al.: Diagnosis of pulmonary embolism. Arch Intern Med 1986; 146: pp. 961-967.
4. den Exter P.L., Hooijer J., Dekkers O.M., et. al.: Risk of recurrent venous thromboembolism and mortality in patients with cancer incidentally diagnosed with pulmonary embolism: a comparison with symptomatic patients. J Clin Oncol 2011; 29: pp. 2405-2409.
5. Sorensen H.T., Mellemkjaer L., Olsen J.H., et. al.: Prognosis of cancers associated with venous thromboembolism. N Engl J Med 2000; 343: pp. 1846-1850.
6. Gladish G.W., Choe D.H., Marom E.M., et. al.: Incidental pulmonary emboli in oncology patients: prevalence, CT evaluation, and natural history. Radiology 2006; 240: pp. 246-255.
7. Sebastian A.J., Paddon A.J.: Clinically unsuspected pulmonary embolism—an important secondary finding in oncology CT. Clin Radiol 2006; 61: pp. 81-85.
8. Cronin C.G., Lohan D.G., Keane M., et. al.: Prevalence and significance of asymptomatic venous thromboembolic disease found on oncologic staging CT. AJR Am J Roentgenol 2007; 189: pp. 162-170.
9. Rita Larici A., Calandriello L., Maggi F., et. al.: Prevalence of incidental pulmonary emboli in oncology patients. Radiology 2007; 245: pp. 921-922. author reply—2
10. Browne A.M., Cronin C.G., English C., et. al.: Unsuspected pulmonary emboli in oncology patients undergoing routine computed tomography imaging. J Thorac Oncol 2010; 5: pp. 798-803.
11. Gladish G.W., Erasmus J.J.: Unsuspected pulmonary emboli in oncology patients undergoing routine computed tomography imaging. J Thorac Oncol 2010; 5: pp. 759-760.
12. Abdel-Razeq H.N., Mansour A.H., Ismael Y.M.: Incidental pulmonary embolism in cancer patients: clinical characteristics and outcome—a comprehensive cancer center experience. Vasc Health Risk Manag 2011; 7: pp. 153-158.
13. Wittram C., Scott J.A.: 18F-FDG PET of pulmonary embolism. AJR Am J Roentgenol 2007; 189: pp. 171-176.
14. Wittram C., Maher M.M., Yoo A.J., et. al.: CT angiography of pulmonary embolism: diagnostic criteria and causes of misdiagnosis. Radiographics 2004; 24: pp. 1219-1238.
15. Di Nisio M., Ferrante N., De Tursi M., et. al.: Incidental venous thromboembolism in ambulatory cancer patients receiving chemotherapy. Thromb Haemost 2010; 104: pp. 1049-1054.
16. Menapace L.A., Peterson D.R., Berry A., et. al.: Symptomatic and incidental thromboembolism are both associated with mortality in pancreatic cancer. Thromb Haemost 2010; 106: pp. 371-378.
17. Revel M.P., Triki R., Chatellier G., et. al.: Is it possible to recognize pulmonary infarction on multisection CT images?. Radiology 2007; 244: pp. 875-882.
18. Blom J.W., Doggen C.J., Osanto S., et. al.: Malignancies, prothrombotic mutations, and the risk of venous thrombosis. JAMA 2005; 293: pp. 715-722.
19. Caine G.J., Stonelake P.S., Lip G.Y., et. al.: The hypercoagulable state of malignancy: pathogenesis and current debate. Neoplasia (New York, NY) 2002; 4: pp. 465-473.
20. Khorana A.A., Francis C.W., Culakova E., et. al.: Thromboembolism is a leading cause of death in cancer patients receiving outpatient chemotherapy. J Thromb Haemost 2007; 5: pp. 632-634.
21. Dentali F., Ageno W., Becattini C., et. al.: Prevalence and clinical history of incidental, asymptomatic pulmonary embolism: a meta-analysis. Thromb Res 2010; 125: pp. 518-522.
22. Goethals I., Smeets P., De Winter O., et. al.: Focally enhanced f-18 fluorodeoxyglucose (FDG) uptake in incidentally detected pulmonary embolism on PET/CT scanning. Clin Nucl Med 2006; 31: pp. 497-498.
23. Ito K., Kubota K., Morooka M., et. al.: Diagnostic usefulness of 18F-FDG PET/CT in the differentiation of pulmonary artery sarcoma and pulmonary embolism. Ann Nucl Med 2009; 23: pp. 671-676.
24. Lee E.J., Moon S.H., Choi J.Y., et. al.: Usefulness of fluorodeoxyglucose positron emission tomography in malignancy of pulmonary artery mimicking pulmonary embolism. ANZ J Surg 2013; 83: pp. 342-347.
25. Franceschi A.M., Matthews R., Mankes S., et. al.: Four chamber FDG uptake in the heart: an indirect sign of pulmonary embolism. Clin Nucl Med 2012; 37: pp. 687-691.
26. Badr A., Joyce J.M., Durick J.: Rim of FDG uptake around a pulmonary infarct on PET/CT in a patient with unsuspected pulmonary embolism. Clin Nucl Med 2009; 34: pp. 285-286.
27. Soussan M., Rust E., Pop G., et. al.: The rim sign: FDG-PET/CT pattern of pulmonary infarction. Insights Imaging 2012; 3: pp. 629-633.
28. Farsad M., Ambrosini V., Nanni C., et. al.: Focal lung uptake of 18F-fluorodeoxyglucose (18F-FDG) without computed tomography findings. Nucl Med Commun 2005; 26: pp. 827-830.
29. Bernard J., Yi E.S.: Pulmonary thromboendarterectomy: a clinicopathologic study of 200 consecutive pulmonary thromboendarterectomy cases in one institution. Hum Pathol 2007; 38: pp. 871-877.
30. Kamel E.M., McKee T.A., Calcagni M.L., et. al.: Occult lung infarction may induce false interpretation of 18F-FDG PET in primary staging of pulmonary malignancies. Eur J Nucl Med Mol Imaging 2005; 32: pp. 641-646.
31. Reid J.H., Murchison J.T.: Acute right ventricular dilatation: a new helical CT sign of massive pulmonary embolism. Clin Radiol 1998; 53: pp. 694-698.
32. Oikawa M., Kagaya Y., Otani H., et. al.: Increased [18F]fluorodeoxyglucose accumulation in right ventricular free wall in patients with pulmonary hypertension and the effect of epoprostenol. J Am Coll Cardiol 2005; 45: pp. 1849-1855.
33. Basu S., Alzeair S., Li G., et. al.: Etiopathologies associated with intercostal muscle hypermetabolism and prominent right ventricle visualization on 2-deoxy-2[F-18]fluoro- d -glucose-positron emission tomography: significance of an incidental finding and in the setting of a known pulmonary disease. Mol Imaging Biol 2007; 9: pp. 333-339.
34. Bokhari S., Raina A., Rosenweig E.B., et. al.: PET imaging may provide a novel biomarker and understanding of right ventricular dysfunction in patients with idiopathic pulmonary arterial hypertension. Circulation 2011; 4: pp. 641-647.