
Rationale and Objectives
To evaluate appropriate utilization rates for computed tomography (CT) pulmonary angiography (CTPA) in a tertiary center emergency department (ED), before and after a health care provider educational intervention.
Materials and Methods
Institutional Review Board–approved retrospective study. Records for 100 consecutive CTPA studies ordered by the ED were retrieved from a radiology database. Appropriateness rates for the studies were determined using information from existing literature (clinical decision rules and society guidelines). Where pretest probability was not performed, it was calculated by the authors. After ED health care provider education regarding appropriateness guidelines through a dedicated lecture and question-and-answer session, appropriateness rates for another 100 consecutive CTPA ordered by the ED were calculated.
Results
In the preeducational intervention, 1% of patients had Wells scores performed, 65% were women, and 29% were age <40 years. Before CTPA, 40% patients had d -dimer testing, 15% of patients had a “negative” d -dimer, 17% had alternative explanations for chest pain, and 76% had low or intermediate pretest probability. Appropriateness rates for CTPA was 7%, and 8% of studies were positive. Postintervention, no Wells scores were performed, 59% were women, and 34% <40 years. Before CTPA, 32% of patients had d -dimer, 16% had a “negative” d -dimer, 22% had alternative explanations for chest pain, and 84% had low or intermediate pretest probability. The appropriateness rate for CTPA was 6% and 10% of studies were positive.
Conclusion
A single educational intervention had no effect on appropriate utilization rates for CTPA. Repeated and sustained educational interventions may help improve imaging ordering pathways through the ED and other departments.
Pulmonary embolism (PE) is a common and potentially fatal condition that is the second most common cause of sudden unexpected death in outpatients after acute coronary syndrome . The annual incidence is estimated at 23 to 69 per 100,000 of the population . Without treatment, PE has a mortality rate of 30% to 35%, but with therapy, the mortality rate drops to less than 5% . For these reasons, emergency department (ED) physicians frequently consider the diagnosis of PE because rapid diagnosis and treatment can significantly diminish the mortality rate and morbidity of this disease.
The clinical diagnosis of PE can be unreliable because many patients are asymptomatic and do not have clinical signs . In addition, patients may present with vague and nonspecific signs and symptoms resulting from hypotension and cardiogenic shock, which overlap with other entities. In the Prospective Investigation Of Pulmonary Embolism Diagnosis (PIOPED) II study, signs of pulmonary hypertension or right heart overload were detected in only 22% of all patients with PE . The diagnosis of PE is also made difficult because there are myriad risk factors.
Imaging overutilization: PE computed tomography
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Demographic Characteristics of 100 Consecutive Patients who had CTPA Performed during Their ED Visit before and after a Health Care Provider Educational Intervention
Demographic Characteristic Pre-educational Intervention Post-educational Intervention_P_ Value ( t test) Mean age (range) 47 (18-93) 49 (18-82) .43 Women (%) 65 59 .47 Patients <40 years (%) 29 34 .54 Patients <40 years with indirect CTV performed (%) 93 97 .33 Patients with clinical pretest probability calculated (prediction rule) (%) 1 0 .32 % of patients with d -dimer performed prior to CTPA 40 32 .31 Patients with a “negative” d -dimer result before CTPA (%) 15 16 .85 Patients with alternative explanation for chest pain before CTPA (%) 17 22 .48 Patients with low pretest probability, manually calculated by radiologists (%) 76 84 .22 Prevalence of venous thromboembolism 8% 10% .81
CTPA, computed tomography pulmonary angiography; ED, emergency department; NS, nonsignificant; test, any diagnostic imaging test (eg, CTPA, ultrasound).
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Criteria Used to Manually Determine the Appropriateness of Each CTPA Study
Criterion Example Clinical gestalt or clinical prediction rule Note from clinician regarding a “sense” that the patient had PE regarded as appropriate.
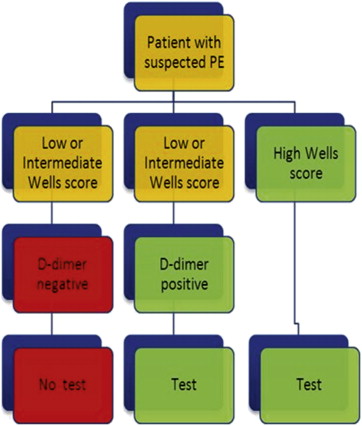
Use of a Wells score or other clinical prediction rule with intermediate or high probability result before CTPA regarded as appropriate. Risk factors or clinical signs Risks (immobilization, cancer, hemoptysis, prior DVT or PE, known thrombotic or hypercoagulable state, signs in one leg [or one leg > other], ECG changes S1Q3T3 pattern), summed using the Wells simplified score. Regarded as inappropriate CTPA if score <2. d -dimer testing Not performing a d -dimer on low or intermediate clinical probability patients regarded as inappropriate. d -dimer level At our institution during this study, an ELISA d -dimer level of <1.6 had a negative predictive value of 99% for DVT. A level of <1.6 was thus regarded as “negative.” Performing CTPA on patients with a negative d -dimer regarded as inappropriate. Results of other diagnostic tests Chest radiography demonstrating pneumonia or pneumothorax, or a normal or low probability V/Q study before the CTPA was regarded as inappropriate if no other risk factors.
CTPA, computed tomography pulmonary angiography; DVT, deep venous thrombosis; ELISA, enzyme-linked immunosorbent assay; PE, pulmonary embolism; V/Q, ventilation perfusion scintigraphy.
Get Radiology Tree app to read full this article<
Educational Intervention
Get Radiology Tree app to read full this article<
Table 3
Subtopics Covered in the 45-Minute Lecture
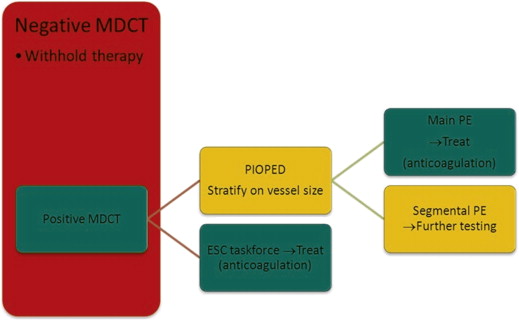
Subtopic Details Background and scope of problem Epidemiology of venous thromboembolic disease; why VTE is difficult to diagnose clinically Clinical decision rules Why we have them; the application of clinical prediction rules to determine the need for advanced testing; their limitations d -dimer testing Description; different types; indications; the usefulness of d -dimer testing in low and intermediate clinical probability patients; contraindications; limitations The imaging modalities that are available to investigate for PE Chest radiography; ultrasound; ventilation perfusion scintigraphy; CTPE; conventional catheter angiography; magnetic resonance imaging; indications and contraindications and limitations CTPA technique Diagnostic performance, pitfalls, limitations, use of indirect CT venography CTPA appearances Acute PE, chronic PE, acute DVT, chronic DVT, direct and indirect signs VTE Other findings on CTPA CT appearances of atelectasis, pneumothorax, pneumonia, pericardial effusion, acute aortic syndromes Radiation issues Radiation exposure; methods to reduce radiation exposure; comparison with other diagnostic tests; the appropriateness of ultrasound imaging in younger and pregnant patients and alternatives to CTPA in certain patient groups Society Guidelines for Appropriate Utilization of CTPA Including PIOPED investigators, PERC, Fleischner Society, ESC task force guidelines with worked examples for low, intermediate, and high pretest probability patients
CT, computed tomography; CTPA, CT pulmonary angiography; DVT, deep venous thrombosis; ESC, European Society of Cardiologists; PE, pulmonary embolism; PERC, Pulmonary Embolism Rule-out Criteria; PIOPED, Prospective Investigators Of Pulmonary Embolism Diagnosis; VTE, venous thromboembolism.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Limitations
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Acknowledgment
Get Radiology Tree app to read full this article<
References
1. Courtney D.M., Sasser H.C., Pincus C.L., Kline J.A.: Pulseless electrical activity with witnessed arrest as a predictor of sudden death from massive pulmonary embolism in outpatients. Resuscitation 2001; 49: pp. 265-272.
2. Kurkciyan I., Meron G., Sterz F., et. al.: Pulmonary embolism as a cause of cardiac arrest: presentation and outcome. Arch Intern Med 2000; 160: pp. 1529-1535.
3. Manfredini R., Portaluppi F., Grandi E., et. al.: Out-of-hospital sudden death referring to an emergency department. J Clin Epidemiol 1996; 49: pp. 865-868.
4. Konstantinides S.: Clinical practice. Acute pulmonary embolism. N Engl J Med 2008; 359: pp. 2804-2813.
5. Dalen J.E.: Pulmonary embolism: what have we learned since Virchow? Natural history, pathophysiology, and diagnosis. Chest 2002; 122: pp. 1440-1456.
6. Dalen J.E.: Pulmonary embolism: what have we learned since Virchow? Treatment and prevention. Chest 2002; 122: pp. 1801-1817.
7. Stein P.D., Beemath A., Matta F., et. al.: Clinical characteristics of patients with acute pulmonary embolism: data from PIOPED II. Am J Med 2007; 120: pp. 871-879.
8. Health status. OECD. Available at: http://stats.oecd.org/index.aspx?DataSetCode=HEALTH_STAT . Accessed October 23, 2012.
9. Fisher E.S., Wennberg D.E., Stukel T.A., et. al.: The implications of regional variations in Medicare spending. Part 1: the content, quality, and accessibility of care. Ann Intern Med 2003; 138: pp. 273-287.
10. Fisher E.S., Wennberg D.E., Stukel T.A., et. al.: The implications of regional variations in Medicare spending. Part 2: health outcomes and satisfaction with care. Ann Int Med 2003; 138: pp. 288-298.
11. Korenstein D., Falk R., Howell E.A., et. al.: Overuse of health care services in the United States: an understudied problem. Arch Intern Med 2012; 172: pp. 171-178.
12. Martin A., Lassman D., Whittle L., Catlin A.: National Healthcare Expenditure Accounts Team. Recession contributes to slowest annual rate of increase in health spending in five decades. Health Aff (Millwood) 2011; 30: pp. 11-22.
13. Dunnick N.R., Applegate K.E., Arenson R.L.: The inappropriate use of imaging studies: a report of the 2004 Intersociety Conference. J Am Coll Radiol 2005; 2: pp. 401-406.
14. Hendee W.R., Becker G., Borgstede J.P., et. al.: Addressing overutilization in medical imaging. Radiology 2010; 257: pp. 240-245.
15. Fazel R., Krumholz H.M., Wang Y., et. al.: Exposure to low-dose ionizing radiation from medical imaging procedures. N Engl J Med 2009; 361: pp. 849-857.
16. Chou R., Qaseem A., Owens D.K., et. al.: Diagnostic imaging for low back pain: advice for high-value health care from the American College of Physicians. Ann Intern Med 2011; 154: pp. 181-189.
17. Larson D.B., Johnson L.W., Schnell B.M., et. al.: Rising use of CT in child visits to the emergency department in the United States, 1995-2008. Radiology 2011; 259: pp. 793-801.
18. Westphalen A.C., Hsia R.Y., Maselli J.H., et. al.: Radiological imaging of patients with suspected urinary tract stones: national trends, diagnoses, and predictors. Acad Emerg Med 2011; 18: pp. 699-707.
19. Welch H.G., Hayes K.J., Frost C.: Repeat testing among Medicare beneficiaries. Arch Intern Med 2012; 172: pp. 1745-1751.
20. Repeat Medical Imaging Classification Neiman Report. Available at: http://www.acr.org/∼/media/ACR/Documents/PDF/Research/Brief%2002/PolicyBriefHPI012013.pdf . Accessed April 17, 2013.
21. Jha S., Ho A., Bhargavan M., et. al.: Imaging evaluation for suspected pulmonary embolism: what do emergency physicians and radiologists say?. AJR Am J Roentgenol 2010; 194: pp. W38-W48.
22. Weiss C.R., Scatarige J.C., Diette G.B., et. al.: CT pulmonary angiography is the first-line imaging test for acute pulmonary embolism: a survey of US clinicians. Acad Radiol 2006; 13: pp. 434-446.
23. Stein P.D., Fowler S.E., Goodman L.R., et. al.: Multidetector computed tomography for acute pulmonary embolism. N Engl J Med 2006; 354: pp. 2317-2327.
24. Mamlouk M.D., vanSonnenberg E., Gosalia R., et. al.: Pulmonary embolism at CT angiography: implications for appropriateness, cost, and radiation exposure in 2003 patients. Radiology 2010; 256: pp. 625-632.
25. Value of ventilation/perfusion scan in acute pulmonary embolism. Results of the prospective investigation of pulmonary embolism diagnosis (PIOPED). The PIOPED Investigators. JAMA 1990; 263: pp. 2753-2759.
26. Stein P.D., Matta F.: Acute pulmonary embolism. Curr Probl Cardiol 2010; 35: pp. 314-376.
27. Shahir K., Goodman L.R., Tali A., et. al.: Pulmonary embolism in pregnancy: CT pulmonary angiography versus perfusion scanning. AJR Am J Roentgenol 2010; 195: pp. W214-W220.
28. Torbicki A., Perrier A., Konstantinides S., et. al., ESC Committee for Practice Guidelines (CPG) : Guidelines on the diagnosis and management of acute pulmonary embolism: the Task Force for the Diagnosis and Management of Acute Pulmonary Embolism of the European Society of Cardiology (ESC). Eur Heart J 2008; 29: pp. 2276-2315.
29. Remy-Jardin M., Pistolesi M., Goodman L.R., et. al.: Management of suspected acute pulmonary embolism in the era of CT angiography: a statement from the Fleischner Society. Radiology 2007; 245: pp. 315-329.
30. Cronin P., Kelly A.: Influence of population prevalences on numbers of false positives: an overlooked entity. Acad Radiol 2011; 18: pp. 1087-1093.
31. Wells P.S., Anderson D.R., Rodger M., et. al.: Derivation of a simple clinical model to categorize patients probability of pulmonary embolism: increasing the models utility with the SimpliRED D-dimer. Thromb Haemost 2000; 83: pp. 416-420.
32. Stein P.D., Woodard P.K., Weg J.G., et. al., PIOPED II Investigators : Diagnostic pathways in acute pulmonary embolism: recommendations of the PIOPED II Investigators. Radiology 2007; 242: pp. 15-21.
33. Le Gal G., Righini M., Roy P.M., et. al.: Prediction of pulmonary embolism in the emergency department: the revised Geneva score. Ann Int Med 2006; 144: pp. 165-171.
34. Miniati M., Piatolesi M.: Assessing the clinical probability of pulmonary embolism. Q J Nucl Med 2001; 45: pp. 287-293.
35. Stein P.D., Sostman H.D., Bounameaux H., et. al.: Challenges in the diagnosis of acute pulmonary embolism. Am J Med 2008; 121: pp. 565-671.
36. Hargett C.W., Tapson V.F.: Clinical probability and D-dimer testing: how should we use them in clinical practice?. Semin Respir Crit Care Med 2008; 29: pp. 15-24.
37. Booz Allen Hamilton. The cost of medical technologies. Maximizing the value of innovation. Available at: http://www.booz.com/media/uploads/TheCostOfMedicalTechnologies.pdf . Accessed November 6, 2012.
38. Sharpe R.E., Levin D.C., Parker L., et. al.: The recent reversal of the growth trend in MRI: a harbinger of the future?. J Am Coll Radiol 2013; March 28
39. Levin D.C., Rao V.M., Parker L.: The recent downturn in utilization of CT: the start of a new trend?. J Am Coll Radiol 2012; 9: pp. 795-798.
40. Dinan M.A., Curtis L.H., Hammill B.G., et. al.: Changes in the use and costs of diagnostic imaging among Medicare beneficiaries with cancer, 1999-2006. JAMA 2010; 303: pp. 1625-1631.
41. Lee D.W., Levy F.: The sharp slowdown in growth of medical imaging: an early analysis suggests combination of policies was the cause. Health Aff (Millwood) 2012; 31: pp. 1876-1884.
42. Chiunda A.B., Mohammed T.L.: Knowledge of ACR thoracic imaging Appropriateness Criteria(R) among trainees: one institution’s experience. Acad Radiol 2012; 19: pp. 635-639.
43. Hardin L.V., Nguyen S.A., Ravenel J.G.: Is e-mail communication effective in changing ordering patterns in the emergency department? A case study of computed tomography for pulmonary embolus. Acad Radiol 2008; 15: pp. 433-437.
44. Bairstow P.J., Mendelson R., Nguyen L.: Reducing inappropriate diagnostic practice through education and decision support. Int J Qual Health Care 2010; 22: pp. 194-200.
45. Blackmore C.C., Mecklenburg R.S., Kaplan G.S.: Effectiveness of clinical decision support in controlling inappropriate imaging. J Am Coll Radiol 2011; 8: pp. 19-25.
46. Carney P.A., Abraham L., Cook A., et. al.: Impact of an educational intervention designed to reduce unnecessary recall during screening mammography. Acad Radiol 2012; 19: pp. 1114-1120.
47. Parent F., Maitre S., Meyer G., et. al.: Diagnostic value of D-dimer in patients with suspected pulmonary embolism: results from a multicentre outcome study. Thromb Res 2007; 120: pp. 195-200.
48. Deonarine P., de Wet C., McGhee A.: Computed tomographic pulmonary angiography and pulmonary embolism: predictive value of a d-dimer assay. BMC Res Notes 2012; 5: pp. 104.
49. Hillman B.J.: Appropriateness. J Am Coll Radiol 2007; 4: pp. 200-201.
50. Blackmore C.C.: Defining quality in radiology. J Am Coll Radiol 2007; 4: pp. 217-223.
51. Raja A.S., Ip I.K., Prevedello L.M., et. al.: Effect of computerized clinical decision support on the use and yield of CT pulmonary angiography in the emergency department. Radiology 2012; 262: pp. 468-474.
52. Elshaug A.G., Bessen T., Moss J.R., et. al.: Addressing “waste” in diagnostic imaging: some implications of comparative effectiveness research. J Am Coll Radiol 2010; 7: pp. 603-613.
53. Bowen S., Johnson K., Reed M.H., et. al.: The effect of incorporating guidelines into a computerized order entry system for diagnostic imaging. J Am Coll Radiol 2011; 8: pp. 251-258.
54. Morgan M.B., Branstetter BFt, Clark C., et. al.: Just-in-time radiologist decision support: the importance of PACS-integrated workflow. J Am Coll Radiol 2011; 8: pp. 497-500.
55. Ip I.K., Schneider L.I., Hanson R., et. al.: Adoption and meaningful use of computerized physician order entry with an integrated clinical decision support system for radiology: ten-year analysis in an urban teaching hospital. J Am Coll Radiol 2012; 9: pp. 129-136.
56. Curry L., Reed M.H.: Electronic decision support for diagnostic imaging in a primary care setting. J Am Med Inform Assoc 2011; 18: pp. 267-270.