
Rationale and Objectives
We compared the effect of iterative model reconstruction (IMR), filtered back projection (FBP), and hybrid iterative reconstruction (HIR) on coronary artery calcium (CAC) scoring.
Materials and Methods
CAC scans of 30 consecutive patients (18 men and 12 women, age 70.1 ± 12.2 years) were reconstructed with FBP, HIR, and IMR, and the image noise was measured on all images. Two radiologists independently measured the CAC scores using semiautomated software, and interobserver agreement was evaluated. Statistical analysis included the Spearman correlation coefficient and Bland-Altman analysis.
Results
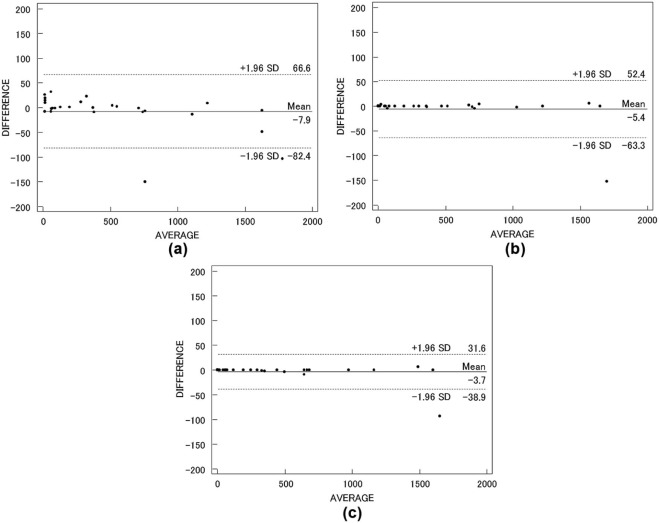
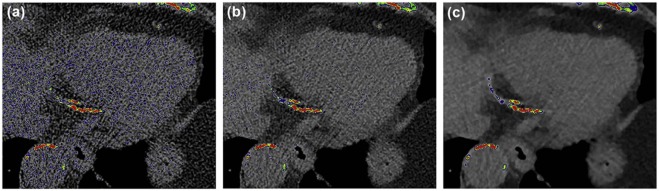
The mean image noise on FBP, HIR, and IMR images was 48.0 ± 7.9, 29.6 ± 4.8, and 9.3 ± 1.3 Hounsfield units, respectively. The difference among all reconstruction combinations was significant ( P < .01). The CAC score on HIR and IMR scans was 4.2% and 8.9% lower, respectively, than the CAC score on FBP images. There was no significant difference in the mean CAC score among the three reconstructions. The interobserver correlation was excellent for all three reconstructions (r 2 = 0.96 FBP, 0.99 HIR, 0.99 IMR); the best Bland-Altman measure of agreement was with IMR, followed by HIR and FBP.
Conclusion
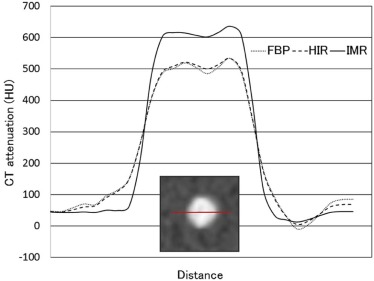
For CAC scoring, IMR can reduce the image noise and blooming artifacts, and consequently lowers the measured CAC score. IMR can lessen measurement variability and yield stable, reproducible measurements.
Introduction
Coronary artery calcium (CAC) is a strong predictor of future cardiovascular events . Multidetector computed tomography (MDCT) is commonly used to assess CAC as part of individual risk evaluations , and CAC scores are obtained at CT screening . As more patients undergo CAC scoring and repeat scanning for treatment monitoring , CAC measurements must yield robust results with low variability to allow meaningful comparisons. A disadvantage of the most commonly used quantification method by Agatston scoring is its limited reproducibility at repeated examinations owing to factors such as the image noise, motion artifacts, and the partial volume effect, etc. . This led to the introduction of two new algorithms, the calcium volume and the calcium mass score , to complement and possibly replace the Agatston score. However, the Agatston score remains the most widely used scoring method because there is strong evidence that it is highly useful in individuals with atherosclerotic heart disease.
As iterative reconstruction (IR) helps to reduce the quantum noise associated with standard convolution-filtered back projection (FBP) reconstruction, it is increasingly integrated in clinical CT studies . Earlier studies indicated that the use of a hybrid IR (HIR) algorithm for cardiac CT, compared to the use of FBP, improves the image quality, allows for a reduction in radiation exposure, and improves the image quality . HIR comprises two denoising components, a sinogram restoration phase that reduces correlated noise and bias artifacts in the projection space, and an iterative denoising process in the image space that reduces the uncorrelated quantum-mottle noise. However, some image noise persists and artifacts may be introduced because of the non-global model of noise reduction. Iterative model reconstruction (IMR), a knowledge-based IR algorithm, is the latest advance in the field of reconstruction techniques. Compared to prior-generation IR, IMR is mathematically more complex, but also more accurate and can provide significantly better image quality than FBP and HIR at cardiac CT . However, the effects of IMR on CAC scoring are still unclear. Renker et al. reported that IR significantly reduced blooming artifacts and calcium volumes on cardiac CT images. If blooming artifacts are reduced by IR, the effects on the detection of small lesions, the assessment of the CAC score, and subsequent risk classification may be possible. We performed phantom and clinical studies to compare the influence of IR on CAC scoring with the effect of standard FBP.
Materials and Methods
Get Radiology Tree app to read full this article<
CT Data Acquisition
Get Radiology Tree app to read full this article<
CT Image Reconstruction
Get Radiology Tree app to read full this article<
CAC Score Measurements
Get Radiology Tree app to read full this article<
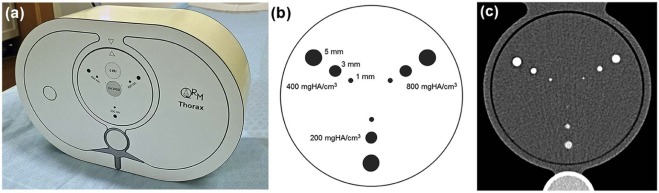
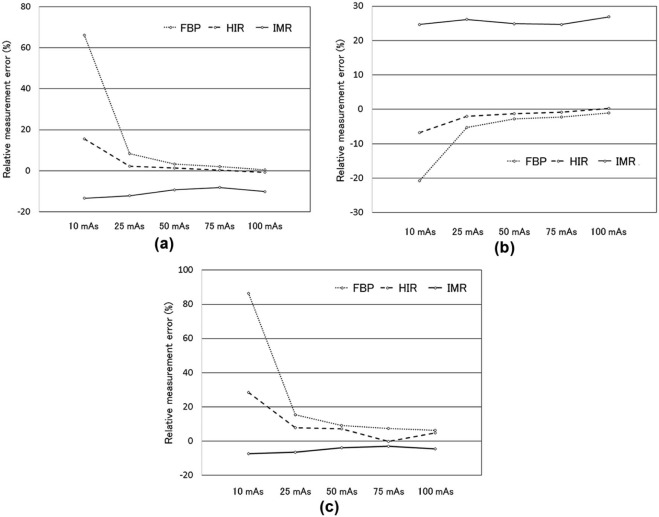
Phantom Study
Get Radiology Tree app to read full this article<
[(measured value−value at250mAs)/value at250mAs]×100. [
(
measured value
−
value at
250
mAs
)
/
value at
250
mAs
]
×
100
.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Clinical Study
Get Radiology Tree app to read full this article<
TABLE 1
Patient Characteristics
Number of patients 30 Age (y) 70.1 ± 12.2 Female/male 12/18 Body weight (kg) 57.5 ± 10.6 Body mass index (kg/m 2 ) 22.7 ± 2.9 Average heart rate (beats/min) 59.0 ± 8.1
Note: Data are mean ± SD.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Phantom Study
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Clinical Study
Get Radiology Tree app to read full this article<
TABLE 2
Results of the Clinical Study
FBP HIR IMR_P_ Value Image noise (HU) 47.3 ± 8.5 27.9 ± 5.1 8.9 ± 1.4 <.01 \* Agatston score Observer 1 495.2 ± 535.6 474.5 ± 529.1 451.6 ± 510.4 .72 Observer 2 503.1 ± 555.5 479.9 ± 542.1 455.2 ± 518.3 .84
FBP, filtered back projection; HIR, hybrid iterative reconstruction; HU, Hounsfield units; IMR, iterative model reconstruction.
Note: Data are mean ± SD.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Greenland P., Alpert J.S., Beller G.A., et. al.: 2010 ACCF/AHA guideline for assessment of cardiovascular risk in asymptomatic adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2010; 56: pp. e50-e103.
2. Wolk M.J., Bailey S.R., Doherty J.U., et. al.: ACCF/AHA/ASE/ASNC/HFSA/HRS/SCAI/SCCT/SCMR/STS 2013 multimodality appropriate use criteria for the detection and risk assessment of stable ischemic heart disease: a report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, American Heart Association, American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Failure Society of America, Heart Rhythm Society, Society for Cardiovascular Angiography and Interventions, Society of Cardiovascular Computed Tomography, Society for Cardiovascular Magnetic Resonance, and Society of Thoracic Surgeons. J Am Coll Cardiol 2014; 63: pp. 380-406.
3. Detrano R., Guerci A.D., Carr J.J., et. al.: Coronary calcium as a predictor of coronary events in four racial or ethnic groups. N Engl J Med 2008; 358: pp. 1336-1345.
4. Burger I.M., Kass N.E., Sunshine J.H., et. al.: The use of CT for screening: a national survey of radiologists’ activities and attitudes. Radiology 2008; 248: pp. 160-168.
5. Raggi P., Davidson M., Callister T.Q., et. al.: Aggressive versus moderate lipid-lowering therapy in hypercholesterolemic postmenopausal women: Beyond Endorsed Lipid Lowering with EBT Scanning (BELLES). Circulation 2005; 112: pp. 563-571.
6. Schmermund A., Achenbach S., Budde T., et. al.: Effect of intensive versus standard lipid-lowering treatment with atorvastatin on the progression of calcified coronary atherosclerosis over 12 months: a multicenter, randomized, double-blind trial. Circulation 2006; 113: pp. 427-437.
7. Yamamoto H., Budoff M.J., Lu B., et. al.: Reproducibility of three different scoring systems for measurement of coronary calcium. Int J Cardiovasc Imaging 2002; 18: pp. 391-397.
8. Callister T.Q., Cooil B., Raya S.P., et. al.: Coronary artery disease: improved reproducibility of calcium scoring with an electron-beam CT volumetric method. Radiology 1998; 208: pp. 807-814.
9. Yoon H.C., Greaser L.E., Mather R., et. al.: Coronary artery calcium: alternate methods for accurate and reproducible quantitation. Acad Radiol 1997; 4: pp. 666-673.
10. Naoum C., Blanke P., Leipsic J.: Iterative reconstruction in cardiac CT. J Cardiovasc Comput Tomogr 2015; 9: pp. 255-263.
11. Oda S., Utsunomiya D., Funama Y., et. al.: A hybrid iterative reconstruction algorithm that improves the image quality of low-tube-voltage coronary CT angiography. AJR Am J Roentgenol 2012; 198: pp. 1126-1131.
12. Oda S., Weissman G., Vembar M., et. al.: Iterative model reconstruction: improved image quality of low-tube-voltage prospective ECG-gated coronary CT angiography images at 256-slice CT. Eur J Radiol 2014; 83: pp. 1408-1415.
13. Oda S., Weissman G., Vembar M., et. al.: Cardiac CT for planning redo cardiac surgery: effect of knowledge-based iterative model reconstruction on image quality. Eur Radiol 2014; 25: pp. 58-64.
14. Renker M., Nance J.W., Schoepf U.J., et. al.: Evaluation of heavily calcified vessels with coronary CT angiography: comparison of iterative andfiltered back projection image reconstruction. Radiology 2011; 260: pp. 390-399.
15. Agatston A.S., Janowitz W.R., Hildner F.J., et. al.: Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol 1990; 15: pp. 827-832.
16. Brown K.M., Zabic S., Koehler T.: Acceleration of ML iterative algorithms for CT by the use of fast start images. Proc SPIE 2012; 8313: pp. 831339.
17. Katsura M., Matsuda I., Akahane M., et. al.: Model-based iterative reconstruction technique for radiation dose reduction in chest CT: comparison with the adaptive statistical iterative reconstruction technique. Eur Radiol 2012; 22: pp. 1613-1623.
18. Singh S., Kalra M.K., Do S., et. al.: Comparison of hybrid and pure iterative reconstruction techniques with conventional filtered back projection: dose reduction potential in the abdomen. J Comput Assist Tomogr 2012; 36: pp. 347-353.
19. den Harder A.M., Willemink M.J., Bleys R.L., et. al.: Dose reduction for coronary calcium scoring with hybrid and model-based iterative reconstruction: an ex vivo study. Int J Cardiovasc Imaging 2014; 30: pp. 1125-1133.
20. Szilveszter B., Elzomor H., Karolyi M., et. al.: The effect of iterative model reconstruction on coronary artery calcium quantification. Int J Cardiovasc Imaging 2016; 32: pp. 153-160.
21. Achenbach S., Ropers D., Mohlenkamp S., et. al.: Variability of repeated coronary artery calcium measurements by electron beam tomography. Am J Cardiol 2001; 87: pp. 210-213. a8
22. Budoff M.J., Kessler P., Gao Y.L., et. al.: The interscan variation of CT coronary artery calcification score: analysis of the Calcium Acetate Renagel Comparison (CARE)-2 study. Acad Radiol 2008; 15: pp. 58-61.
23. Horiguchi J., Yamamoto H., Hirai N., et. al.: Variability of repeated coronary artery calcium measurements on low-dose ECG-gated 16-MDCT. AJR Am J Roentgenol 2006; 187: pp. W1-W6.