
Rationale and Objectives
Mammography contributes to the improvement of breast carcinoma survival through early detection and treatment of breast lesions. The basal-like phenotype has been found to be an independent poor prognostic factor for breast cancer. The aim of this study was to determine the mammographic correlates of the basal-like phenotype of invasive breast cancer, and to more precisely predict patient outcome and those individuals who will be responsive to a specific therapeutic regimen.
Materials and Methods
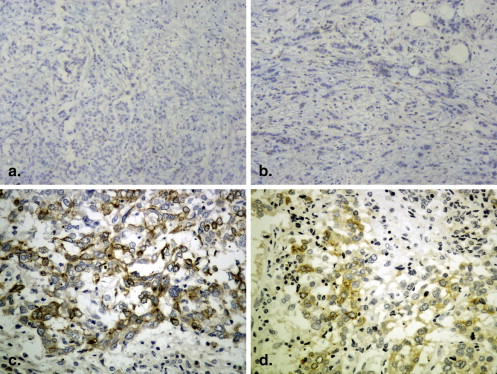
The mammographic findings in 267 patients with operable breast cancer were correlated with the basal-like subtype identified using immunohistochemical assessment of breast cancer cases, including estrogen receptor, progesterone receptor, HER-2/neu status, cytokeratin (CK5/6), and epidermal growth factor receptor.
Results
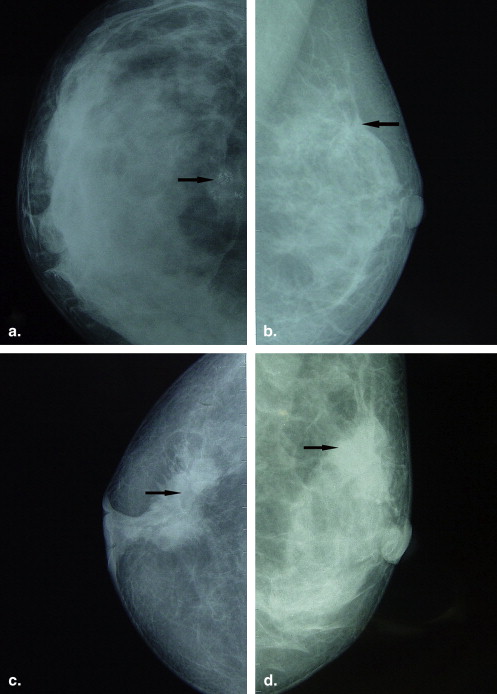
Of the 267 invasive breast cancers, 40 (15%) were of the basal-like phenotype. Basal-phenotype tumors were significantly more likely to manifest as a mass ( P = .002), most of which were indistinct margin ( P = .035), at mammography, and architecture distortion at mammography ( P = .002).
Conclusion
The mammographic appearances of basal-like tumors, more mass and architecture distortion, suggest more rapid carcinogenesis. Additional studies are warranted to further refine prognosis, and to optimize treatment in patients with basal-like breast cancer.
Analysis of breast cancer tissue with DNA microarrays has categorized breast carcinoma into the following five distinct subtypes: luminal A (estrogen receptor [ER] positive and/or progesterone receptor [PR] positive, human epidermal growth factor receptor 2 [HER-2/neu) negative], luminal B (ER positive and/or PR positive, HER-2/neu positive), HER-2/neu overexpression (ER negative, PR negative, HER-2/neu positive), basal-like (ER negative, PR negative, HER-2/neu negative, cytokeratin 5 and 6 [CK5/6] positive and/or epidermal growth factor receptor [EGFR] positive) and normal breast-like tumors. Although this classification system is based on extensive genetic profiling assays, a simplified method of classification (based on ER, PR, HER-2/neu, CK5/6, and EGFR status) is appealing and more clinically useful. The basal-like subtype is associated with aggressive histology, poor prognosis, unresponsiveness to the usual endocrine therapies, and shorter survival . The pathways that drive proliferation of these tumors are still poorly understood; however, after they have been elucidated, targeted agents can be developed, which could result in better outcomes for patients with basal-like tumors.
Several studies have attempted to evaluate and interpret the clinical perspective of the relationship between mammographic features and HER-2/neu overexpression in breast carcinomas, and shown that mammographic calcifications are correlated with HER-2/neu overexpression in breast carcinomas . Furthermore, the clinical perspective of the relationship between mammographic calcifications and the expression of selected biological markers, such as ER, PR, EGFR, Bax, Fas, Bcl-2, and DNA fragmentation factor in breast carcinomas have been interpreted .
Get Radiology Tree app to read full this article<
Materials and methods
Patients
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Mammography
Get Radiology Tree app to read full this article<
Basal-like Breast Carcinoma Tissues
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Correlation between Basal-like Breast Carcinomas and Clinicopathological Parameters
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Difference of Clinicopathological Characteristics between Basal-like and Non–basal-like Breast Cancers
Tumor Phenotype (%) Characteristics_n_ Basal-like ( n = 40) Non–basal-like ( n = 227)P Value Age at diagnosis ≤35 34 14 (35%) 20 (9%) 36–49 126 15 (38%) 111 (49%) ≥50 107 11 (27%) 96 (42%) .001 Menopause status Premenopausal 147 31 (78%) 116 (51%) Postmenopausal 120 9 (22%) 111 (49%) .003 Histology Ductal 218 36 (90%) 182 (80%) Lobular 22 2 (5%) 20 (9%) Others 27 2 (5%) 2 5(11%) .33 T stage T1 108 9 (23%) 99 (44%) T2 136 20 (50%) 116 (51%) T3 23 11 (27%) 12 (5%) .001 Nodal status Negative 176 25 (62%) 151 (67%) Positive 91 15 (38%) 76 (33%) .75 Tumor grade 1 90 10 (25%) 80 (35%) 2 116 14 (35%) 102 (45%) 3 61 16 (40%) 45 (20%) .019
Get Radiology Tree app to read full this article<
Correlation between Mammographic Features and Basal-like Phenotype
Get Radiology Tree app to read full this article<
Table 2
Association between Mammographic Features and Basal-like Breast Cancers
Tumor Phenotype (%) Mammographic Findings Basal-like ( n = 40) Non–basal-like ( n = 227)P Value Mass + 22 (55%) 65 (29%) − 18 (45%) 162 (71%) .002 Calcification + 14 (35%) 87 (38%) .82 − 26 (65%) 140 (62%) Architectural distortion + 13 (33%) 28 (12%) − 27 (67%) 199 (88%) .002 Asymmetric density + 3 ( 8%) 12 (5%) − 37 (92%) 215 (95%) .85
Get Radiology Tree app to read full this article<
Correlation between Shape, Margin, Density, and Associated Findings of Mass on Mammography and Basal-like Phenotype
Get Radiology Tree app to read full this article<
Table 3
Associations between Shape, Margin, Density, and Associated Findings of Mass on Mammography and Basal-like Breast Cancers
Tumor Phenotypes (%) Mammographic Mass Features Basal-like ( n = 22) Non–basal-like ( n = 65)P Value Mass shape Round 5 (23%) 16 (25%) .99 Oval 4 (18%) 21 (32%) .48 Lobulated 4 (18%) 13 (20%) .87 Irregular 9 (41%) 15 (23%) .35 Mass margin Circumscribed 2 ( 9%) 11 (17%) .66 Microlobulated 5 (23%) 17 (26%) .89 Obscured 3 (14%) 10 (15%) .86 Indistinct 8 (36%) 6 (9%) .035 Spiculated 4 (18%) 21 (32%) .48 Density High 9 (41%) 25 (38%) .89 Equal 10 (45%) 30 (46%) .97 Low 3 (14%) 10 (16%) .86 Associated findings Calcifications 14 (63%) 25 (38%) .32 Architectural distortion 3 (14%) 7 (11%) .99 Skin retraction 2 (9%) 5 (8%) .99
Get Radiology Tree app to read full this article<
Correlation between Mammographic Calcification Features and Basal-like Phenotype
Get Radiology Tree app to read full this article<
Table 4
Associations between Mammographic Calcification Features and Basal-like Breast Cancers
Tumor Phenotype (%) Mammographic Calcification Features Basal-like ( n = 14) Non–basal-like ( n = 87)P Value Distribution Clustered 6 (42%) 34 (39%) .99 Segmental 3 (21%) 13 (15%) .89 Regional 1 (7%) 9 (10%) .99 Linear 1 (7%) 16 (18%) .60 Diffuse 3 (21%) 15 (17%) .99 Morphologic aspects Pleomorphic 9 (64%) 33 (38%) .38 Fine linear 2 (14%) 21 (24%) .75 Punctate 2 (14%) 19 (22%) .86 Coarse 1 (7%) 14 (16%) .72
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Sorlie T., Tibshirani R., Parker J., et. al.: Repeated observation of breast tumor subtypes in independent gene expression data sets. Proc Natl Acad Sci U S A 2003; 100: pp. 8418-8423.
2. Livasy C.A., Karaca G., Nanda R., et. al.: Phenotype evaluation of the basal-like subtype of invasive breast carcinoma. Mod Pathol 2006; 19: pp. 264-271.
3. Karamouzis M.V., Likaki-Karatza E., Ravazoula P., et. al.: Non-palpable breast carcinomas: correlation of mammographically detected malignant-appearing microcalcifications and molecular prognostic factors. Int J Cancer 2002; 102: pp. 86-90.
4. Evans A.J., Pinder S.E., Ellis I.O., et. al.: Correlations between the mammographic features of ductal carcinoma in situ (DCIS) and C-erbB-2 oncogene expression. Clin Radiol 1994; 49: pp. 559-562.
5. Seo B.K., Pisano E.D., Kuzimak C.M., et. al.: Correlation of HER-2/neu overexpression with mammography and age distribution in primary breast carcinomas. Acad Radiol 2006; 13: pp. 1211-1218.
6. Wang X., Chao L., Chen L., et. al.: Correlation of mammographic calcifications with HER-2/neu overexpression in primary breast carcinomas. J Digit Imaging 2008; 21: pp. 170-176.
7. Likaki-Karatza E., Ravazoula P., Androutsopoulos G., et. al.: Correlation of mammographic appearance and molecular prognostic factors in high-grade breast carcinomas. Eur J Gynaecol Oncol 2006; 27: pp. 39-41.
8. Ildefonso C., Vazquez J., Guinea O., et. al.: The mammographic appearance of breast carcinomas of invasive ductal type: relationship with clinicopathological parameters, biological features and prognosis. Eur J Obstet Gynecol Reprod Biol 2008; 136: pp. 224-231.
9. Luck A.A., Evans A.J., James J.J., et. al.: Breast carcinoma with basal phenotype: mammographic findings. AJR Am J Roentgenol 2008; 191: pp. 346-351.
10. Yang W.T., Dryden M., Broglio K., et. al.: Mammographic features of triple receptor-negative primary breast cancers in young premenopausal women. Breast Cancer Res Treat 2008; 111: pp. 405-410.
11. Le Doussal V., Tubiana-Hulin M., Friedman S., et. al.: Prognostic value of histologic grade nuclear components of Scarff-Bloom-Richardson (SBR): an improved score modification based on a multivariate analysis of 1262 invasive ductal breast carcinomas. Cancer 1989; 64: pp. 1914-1921.
12. Greene F.I., Page D.I., Fleming I.D.: AJCC cancer staging manual.6th ed.2002.SpringerNew York
13. Obenauer S., Hermann K.P., Grabbe E.: Applications and literature review of the BI-RADS classification. Eur Radiol 2005; 15: pp. 1027-1036.
14. American College of Radiology: Breast imaging reporting and data system (BI-RADS).4th ed.2003.American College of RadiologyReston, VA
15. Cheang M.C., Voduc D., Bajdik C., et. al.: Basal-like breast cancer defined by 5 biomarkers has superior prognostic value than triple-negative phenotype. Clin Cancer Res 2008; 14: pp. 1368-1376.
16. Nielsen T.O., Hsu F.D., Jensen K., et. al.: Immunohistochemical and clinical characterization of the basal-like subtype of invasive breast carcinoma. Clin Cancer Res 2004; 10: pp. 5367-5374.
17. Carey L.A., Perou C.M., Livasy C.A., et. al.: Race, breast cancer subtypes, and survival in the Carolina Breast Cancer Study. JAMA 2006; 295: pp. 2492-2502.
18. Bertucci F., Finetti P., Cervera N., et. al.: How basal are triple-negative breast cancers?. Int J Cancer 2008; 123: pp. 236-240.
19. Bidard F.C., Conforti R., Boulet T., et. al.: Does triple negative phenotype accurately identify basal-like tumour? An immunohistochemical analysis based on 143 ‘triple-negative’ breast cancers. Ann Oncol 2007; 18: pp. 1285-1286.
20. Tan D.S., Marchio C., Jones R.L., et. al.: Triple negative breast cancer molecular profiling and prognostic impact in adjuvant anthracycline-treated patients. Breast Cancer Res Treat 2008; 111: pp. 27-44.
21. Bauer K.R., Brown M., Cress R.D., et. al.: Descriptive analysis of estrogen receptor (ER)-negative, progesterone receptor (PR)-negative, and HER2-negative invasive breast cancer, the so-called triple-negative phenotype: a population-based study from the California Cancer Registry. Cancer 2007; 109: pp. 1721-1728.
22. Dent R., Trudeau M., Pritchard K.I., et. al.: Triple-negative breast cancer: clinical features and patterns of recurrence. Clin Cancer Res 2007; 13: pp. 4429-4434.
23. Brown M., Tsodikov A., Bauer K.R., et. al.: The role of human epidermal growth factor receptor 2 in the survival of women with estrogen and progesterone receptor-negative, invasive breast cancer: the California Cancer Registry, 1999–2004. Cancer 2008; 112: pp. 737-747.
24. Lund M.J., Butler E.N., Bumpers H.L., et. al.: High prevalence of triple-negative tumors in an urban cancer center. Cancer 2008; 113: pp. 608-615.
25. Rakha E.A., El-Rehim D.A., Paish C., et. al.: Basal phenotype identifies a poor prognostic subgroup of breast cancer of clinical importance. Eur J Cancer 2006; 42: pp. 3149-3156.
26. Tabar L., Chen H.-H., Duffy S.W., et. al.: A novel method for prediction of long-term outcome of women with T1a, T1b, and 10–14 mm invasive breast cancers: a prospective study. Lancet 2000; 355: pp. 429-433.
27. Thurfjell E., Thurfjell M.G., Lindgren A.: Mammographic finding as predictor of survival in 1–9 mm invasive breast cancers. Worse prognosis for cases presenting as calcifications alone. Breast Cancer Res Treat 2001; 67: pp. 177-180.
28. Broeders M.M., Onland-Moret N.C., Rijken H.M., et. al.: Use of previous screening mammograms to identify features indicating cases that would have a possible gain in prognosis following earlier detection. Eur J Cancer 2003; 39: pp. 1770-1775.
29. Yankaskas B.C., Schell M.J., Bird R.E., et. al.: Reassessment of breast cancers missed during routine screening mammography: a community-based study. Am J Roentgenol 2001; 177: pp. 535-541.
30. Venkatesan A., Chu P., Kerlikowske K., et. al.: Positive predictive value of specific mammographic findings according to reader and patient variables. Radiology 2009; 250: pp. 648-657.