
Rationale and Objectives
The practice of moonlighting by trainees is a longstanding controversy; however, the resident point of view remains distinctly underrepresented in the radiology literature. We report the resident perspective on the moonlighting practices of radiology trainees.
Methods
Survey data were collected from resident members of the Association of University Radiologists representing 84 training programs in the United States to assess their routine and extracurricular clinical responsibilities. Descriptive statistics were used to analyze these data.
Results
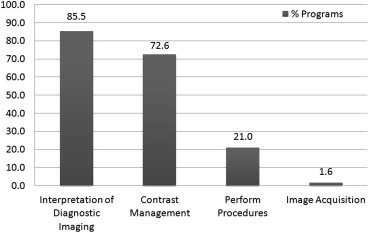
Moonlighting is practiced by radiology trainees at nearly three-fourths of the programs represented in this survey. Interpreting diagnostic imaging (85.5%) and monitoring contrast administrations (72.6%) are the most common duties performed. Twenty-one percent of moonlighting trainees perform procedures (excluding diagnostic fluoroscopy) in their extracurricular positions; of these, most (61.5%) are without attending supervision. Most trainees that moonlight spend 1 to 10 hours weekly doing so while averaging a 59-hour workweek at their primary jobs.
Conclusions
The clinical duties of moonlighting trainees may be more diverse than has been previously recognized. Although major discrepancies between overnight radiology trainee interpretations and attending final interpretations have been shown to be infrequent, the consequences of trainees performing procedures and monitoring adverse contrast reactions without attending supervision are unknown. The financial and professional benefits of moonlighting must be weighed against the potential for harm. Our data suggest that most moonlighting radiology trainees operate within the Accreditation Council for Graduate Medical Education–mandated 80-hour weekly work limit; the mandatory 8-hour break between shifts and 24-hour continuous duty limit may pose logistical challenges.
Resident physicians are a heavily leveraged breed. Eighty-six percent of the US medical school class of 2011 will graduate with medical student loans, with a median amount of $162,000 ; one-third will have incurred $200,000 or more in medical education debt. As interest accrues over a 25- to 30-year repayment period, the true financial burden of medical education becomes much higher. It has been shown that residents have fewer assets, greater consumer debt, and smaller retirement funds when compared to members of the general public with post-college degrees . A 2002 survey of internal medicine trainees found that 52% had insufficient funds to purchase textbooks and work-related equipment, and that nearly one-third could not afford the required fees for their board certification exam . Similarly, many radiology residents bear considerable responsibility for American Board of Radiology certification fees, licensing costs, and radiologic-pathologic course (American Institute for Radiologic Pathology) expenses, which may amount to 16% of their annual salary .
In light of these circumstances, many resident physicians may perceive an acute need for supplementary income. Indebtedness is highly associated with the pursuit of moonlighting opportunities . However, in addition to its economic benefits , some authors have emphasized the educational value of the practical experience gained through these additional responsibilities .
Get Radiology Tree app to read full this article<
Methods
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
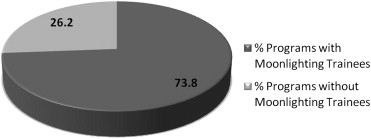
Table 1
Factors Influencing the Decision not to Moonlight
Barriers to Moonlighting_n_ % ∗ Market forces 16 72.7 Lack of interest 3 13.6 Administrative disapproval 12 54.5 Total 31 † N/A
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Responses from Radiology Programs with Moonlighting Opportunities for Trainees
n %Department stance on moonlighting Encouraged. 25 40.3 Allowed, but not encouraged. 36 58.1 Forbidden, but happens anyway 1 1.6 Total 62 100.0Equal opportunities within a given class? Yes 51 82.3 No 11 17.7 Total 62 100.0Moonlighting at what type of facility? Inpatient 13 21.0 Outpatient 17 27.4 Hybrid 6 9.7 Both 26 41.9 Total 62 100.0Procedures while moonlighting? None 49 79.0 Unsupervised 8 12.9 Supervised 5 8.1 Total 62 100.0Hours spent moonlighting weekly? 1–10 49 79.0 11–20 12 19.4 21+ 1 1.6 Total 62 100.0Residents provide own liability insurance? No 54 87.1 Yes 7 11.3 Unsure 1 1.6 Total 62 100.0
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Supplementary Data
Get Radiology Tree app to read full this article<
Appendix
Get Radiology Tree app to read full this article<
References
1. Association of American Medical Colleges. FIRST analysis of AAMC 2011 Graduation Questionnaire (GQ) data. Available at: www.aamc.org/first . Accessed November 26, 2011.
2. Teichman J.M., Cecconi P.P., Bernheim B.D., et. al.: How do residents manage personal finances?. Am J Surg 2005; 189: pp. 134-139.
3. Collier V.U., McCue J.D., Markus A., et. al.: Stress in medical residency: status quo after a decade of reform?. Ann Intern Med 2002; 136: pp. 384-390.
4. Tilak G.S., Baker S.R.: Self-subsidization of educational expenses by senior radiology residents. Acad Radiol 2007; 14: pp. 105-109.
5. Baker S.R., Romero M.J., Patel A., et. al.: Internal and external moonlighting by radiology trainees: a survey of the extent of participation by current residents and fellows. Acad Radiol 2009; 16: pp. 1029-1033.
6. Greco R.S., Donetz A.P., Brolin R.E., et. al.: The influence of debt, moonlighting, practice, oversupply and gender on career development of residents in university and independent training programs. Surg Gynecol Obstet 1987; 165: pp. 19-24.
7. Li J., Tabor R., Martinez M.: Survey of moonlighting practices and work requirements of emergency medicine residents. Am J Emerg Med 2000; 18: pp. 147-151.
8. Kazzi A.A., Langdorf M.I., Brillman J., et. al.: Emergency medicine residency applicant educational debt: relationship with attitude toward training and moonlighting. Acad Emerg Med 2000; 7: pp. 1399-1407.
9. Silliman R.A., Dittus R.S., Velez R., et. al.: Debt, moonlighting, and career decisions among internal medicine residents. J Med Educ 1987; 62: pp. 463-469.
10. Hunt K.R., Hillman B.J., Witzke D.B.: Moonlighting during the radiology residency. Invest Radiol 1992; 27: pp. 978-983.
11. Culler S.D., Bazzoli G.J.: The moonlighting decisions of resident physicians. J Health Econ 1985; 4: pp. 283-292.
12. Bazzoli G.J., Culler S.D.: Factors affecting residents’ decisions to moonlight. J Med Educ 1986; 61: pp. 797-802.
13. Moss A.J.: Moonlighting house officers: the silent majority. N Engl J Med 1984; 311: pp. 1375-1377.
14. Baldwin D.C., Daugherty S.R.: Moonlighting and indebtedness reported by PGY2 residents: it’s not just about money!. Acad Med 2002; 77: pp. S36-S38.
15. McCue J.D., Janiszewski M., Stickley W.T.: Residents’ views of the value of moonlighting. Arch Intern Med 1990; 150: pp. 1511-1513.
16. Mainiero M.B., Woodfield C.A.: Resident moonlighting in radiology. J Am Coll Radiol 2008; 5: pp. 766-769.
17. Cohen S.N., Leeds M.P.: The moonlighting dilemma. Balancing education, service, and quality care while limiting risk exposure. JAMA 1989; 262: pp. 529-531.
18. Berlin L.: Liability of the moonlighting resident. AJR Am J Roentgenol 1998; 171: pp. 565-567.
19. Chisholm C.D.: The moonlighting paradox. Am J Emerg Med 2000; 18: pp. 224-226.
20. Accreditation Council for Graduate Medical Education. Report of the ACGME Work Group on Resident Duty Hours. Available at: http://www.acgme.org/acWebsite/dutyhours/dh_wkgroupreport611.pdf . Accessed June 28, 2012.
21. Accreditation Council for Graduate Medical Education. Common Program Requirements. Available at: http://www.acgme-2010standards.org/pdf/Common_Program_Requirements_07012011.pdf . Accessed June 28, 2012.
22. Martini S., Arfken C.L., Churchill A., et. al.: Burnout comparison among residents in different medical specialties. Acad Psychiatry 2004; 28: pp. 240-242.
23. Wang C.L., Cohan R.H., Ellis J.H., et. al.: Frequency, management, and outcome of extravasation of nonionic iodinated contrast medium in 69,657 intravenous injections. Radiology 2007; 243: pp. 80-87.
24. Wang C.L., Cohan R.H., Ellis J.H., et. al.: Frequency, outcome, and appropriateness of treatment of nonionic iodinated contrast media reactions. AJR Am J Roentgenol 2008; 191: pp. 409-415.
25. West C.P., Shanafelt T.D., Kolars J.C.: Quality of life, burnout, educational debt, and medical knowledge among internal medicine residents. JAMA 2011; 306: pp. 952-960.
26. Drentea P., Lavrakas P.: Over the limit: the association among health, race and debt. Social Sci Med 2000; 50: pp. 517-529.
27. Reading R., Reynolds S.: Debt, social disadvantage and maternal depression. Soc Sci Med 2001; 53: pp. 441-453.
28. Paul K., Batinic B.: The need for work: Jahoda’s latent functions of employment in a representative sample of the German population. J Organizational Behav 2010; 31: pp. 45-64.
29. Ennis N.E., Hobfoll S.E., Schröder K.E.: Money doesn’t talk, it swears: how economic stress and resistance resources impact inner-city women’s depressive mood. Am J Community Psychol 2000; 28: pp. 149-173.
30. Hoelzl E., Pollai M., Kamleitner B.: Experience, prediction and recollection of loan burden. J Econ Psychol 2009; 30: pp. 446-454.
31. Sinclair R., Sears L., Probst T., et. al.: A multilevel model of economic stress and employee well-being.Houdmont J.Leka S.Contemporary occupational health psychology. Global perspectives on research and practice.2010.Wiley-BlackwellWest Sussex:pp. 1-20.
32. Selenko E., Batinic B.: Beyond debt. A moderator analysis of the relationship between perceived financial strain and mental health. Soc Sci Med 2011; 73: pp. 1725-1732.
33. Jahoda M.: Employment and unemployment. A socialepsychological analysis.1982.Cambridge University PressCambridge
34. Wechsler R.J., Spettell C.M., Kurtz A.B., et. al.: Effects of training and experience in interpretation of emergency body CT scans. Radiology 1996; 199: pp. 717-720.
35. Carney E., Kempf J., DeCarvalho V., et. al.: Preliminary interpretations of after-hours CT and sonography by radiology residents versus final interpretations by body imaging radiologists at a level 1 trauma center. AJR Am J Roentgenol 2003; 181: pp. 367-373.
36. Strub W.M., Vagal A.A., Tomsick T., et. al.: Overnight resident preliminary interpretations on CT examinations: should the process continue?. Emerg Radiol 2006; 13: pp. 19-23.
37. Stevens K.J., Griffiths K.L., Rosenberg J., et. al.: Discordance rates between preliminary and final radiology reports on cross-sectional imaging studies at a level 1 trauma center. Acad Radiol 2008; 15: pp. 1217-1226.
38. Cooper V.F., Goodhartz L.A., Nemcek A.A., et. al.: Radiology resident interpretations of on-call imaging studies: the incidence of major discrepancies. Acad Radiol 2008; 15: pp. 1198-1204.
39. Velmahos G.C., Fili C., Vassiliu P., et. al.: Around-the-clock attending radiology coverage is essential to avoid mistakes in the care of trauma patients. Am Surg 2001; 67: pp. 1175-1177.
40. Lal N.R., Murray U.M., Eldevik O.P., et. al.: Clinical consequences of misinterpretations of neuroradiologic CT scans by on-call radiology residents. AJNR Am J Neuroradiol 2000; 21: pp. 124-129.
41. Chung J.H., Strigel R.M., Chew A.R., et. al.: Overnight resident interpretation of torso CT at a level 1 trauma center an analysis and review of the literature. Acad Radiol 2009; 16: pp. 1155-1160.