
Rationale and Objectives
The relationship between chronic obstructive pulmonary disease (COPD) and atherosclerosis has been suggested; this association may relate to systemic inflammation and endothelial dysfunction, which can lead to alteration of small pulmonary vessels. The relationship between atherosclerosis and small pulmonary vessel alteration, however, has not been assessed in COPD patients. We tested the hypothesis that the severity of thoracic aortic calcification measured by computed tomography (CT) would be associated with the total cross-sectional area of small pulmonary vessels (CSA) on CT images.
Materials and Methods
The study was approved by the institutional review board and was Health Insurance Portability and Accountability Act–compliant. Informed consent was waived. For 51 COPD patients enrolled in the National Heart, Lung, and Blood Institute Lung Tissue Research Consortium, we calculated the percentage of total CSAs of less than 5 mm 2 for the total lung area (%CSA<5). Thoracic aortic calcification, quantified by modified Agatston score, was measured. The correlations between thoracic aortic calcification score and %CSA<5, pulmonary function, and extent of emphysema were evaluated. Multiple linear regression analysis using aortic calcification score as the dependent outcome was also performed.
Results
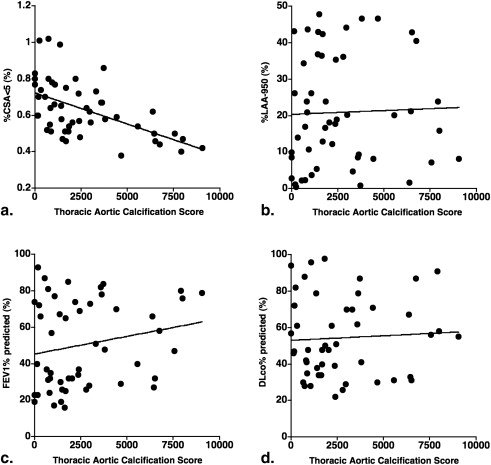
The %CSA<5 had a significant negative correlation with the thoracic aortic calcification score ( r = −0.566, P < .0001). Multiple linear regression analysis showed significant correlation between the aortic calcification score and %CSA<5 ( P < .0001) independent of age, pack-years, extent of emphysema, and FEV1%.
Conclusions
Atherosclerosis, assessed by aortic calcification, is associated with the small pulmonary vascular alteration in COPD. Systemic inflammation and endothelial dysfunction may cause the close relationship between atherosclerosis and small pulmonary vessel alteration.
Chronic obstructive pulmonary disease (COPD) is a systemic inflammatory disorder in which inflammation may be associated to the development of cardiovascular diseases . Although the underlying mechanisms remain unknown, cardiovascular disease contributes significantly to morbidity and mortality in COPD . Atherosclerosis is the principal cause of cardiovascular diseases, including coronary heart disease, stroke, and peripheral vascular disease , and it is thought to be associated with systemic inflammation and endothelial dysfunction . Prior investigations suggested that systemic inflammation in COPD may promote atherosclerosis , and recent studies have reported relationships between atherosclerosis and COPD .
The development of arterial calcification is an active process seen at all stages of atherosclerotic plaque development, and is closely associated with vascular injury . Many researchers have reported the relationship between aortic calcification and an increased risk of cardiovascular events . Patients with calcification in the thoracic aorta have 3.8 times the relative risk for obstructive coronary artery disease independent of age . In addition, a recent study showed that the severity of thoracic aortic calcification measured by computed tomography (CT) strongly correlates with inflammatory markers such as interleukin-6 .
Get Radiology Tree app to read full this article<
Methods
Subjects
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Multislice CT Scanning
Get Radiology Tree app to read full this article<
CT Measurement of Small Pulmonary Vessels
Get Radiology Tree app to read full this article<
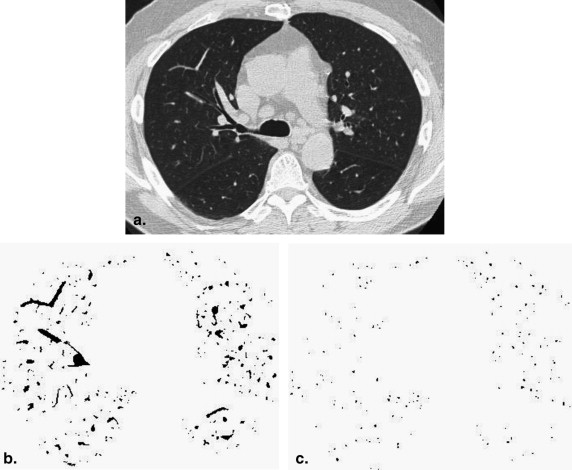
Get Radiology Tree app to read full this article<
CT Measurement of the Thoracic Aortic Calcification
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Demographics, Pulmonary Function, and CT Measurements ( n = 51)
Mean SD Range Age (y) 66 9 47–82 Gender, % female (%) 42.8 BMI 26.3 4.6 16.5–41.8 Pack-years 48.0 30.8 1–128 FEV1 (l) 1.42 0.77 0.5–3.9 FVC (l) 3.0 1.1 0.9–5.8 FEV1% predicted (%) 50.4 23.7 16.0–93.0 FEV1/FVC 0.46 0.15 0.23–0.69 DLco% predicted (%) 54.4 21.9 22.0–98.0 %CSA<5 (%) 0.63 0.15 0.38–1.02 %LAA-950 (%) 20.9 15.1 0.4–47.9
SD, standard deviation; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; DL CO , diffusing capacity of the lung for carbon monoxide; BMI, body mass index; %CSA<5, percentage of total lung area taken up by the cross-sectional area of pulmonary vessels <5 mm 2 ; %LAA-950, CT measurement of the percentage of low attenuation area less than −950 HU, defined as emphysema.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Correlations of Aortic Calcification Score with Continuous Variables (Spearman’s Rank Correlations) ( n = 51)
Aortic Calcification Score_r__P_ Age 0.508 .0001 BMI −0.001 .992 Pack-years 0.183 .197 FEV1% predicted 0.201 .156 DLco% predicted 0.014 .925 %CSA<5 −0.566 <.0001 %LAA-950 0.119 .405
SD, standard deviation; FEV1, forced expiratory volume in 1 second; DL CO , diffusing capacity of the lung for carbon monoxide; BMI, body mass index; %CSA<5, percentage of total lung area taken up by the cross-sectional area of pulmonary vessels <5 mm 2 ; %LAA-950, CT measurement of the percentage of low attenuation area less than −950 HU, defined as emphysema.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Multivariate Analysis of Aortic Calcification Score ( n = 51)
Partial Correlation Coefficient_P_ Value Age 0.351 .0049 Gender −0.053 .838 BMI −0.061 .672 Pack-years 0.007 .968 FEV1% predicted −0.044 .886 DLco% predicted 0.084 .601 %CSA<5 −0.564 <.0001 Total lung area −0.175 .223 %LAA-950 −0.223 .172
SD, standard deviation; FEV1, forced expiratory volume in 1 second; DL CO , diffusing capacity of the lung for carbon monoxide; BMI, body mass index; %CSA<5, percentage of total lung area taken up by the cross-sectional area of pulmonary vessels <5 mm 2 ; %LAA-950, CT measurement of the percentage of low attenuation area less than −950 HU, defined as emphysema.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Gan W.Q., Man S.F., Senthilselvan A., et. al.: Association between chronic obstructive pulmonary disease and systemic inflammation: a systematic review and a meta-analysis. Thorax 2004; 59: pp. 574-580.
2. Donaldson G.C., Seemungal T.A., Patel I.S., et. al.: Airway and systemic inflammation and decline in lung function in patients with COPD. Chest 2005; 128: pp. 1995-2004.
3. Pinto-Plata V.M., Müllerova H., Toso J.F., et. al.: C-reactive protein in patients with COPD, control smokers and non-smokers. Thorax 2006; 61: pp. 23-28.
4. Palange P., Testa U., Huertas A., et. al.: Circulating haemopoietic and endothelial progenitor cells are decreased in COPD. Eur Respir J 2006; 27: pp. 529-541.
5. Sin D.D., Man S.F.: Why are patients with chronic obstructive pulmonary disease at increased risk of cardiovascular diseases? The potential role of systemic inflammation in chronic obstructive pulmonary disease. Circulation 2003; 107: pp. 1514-1519.
6. Man S.F., Connett J.E., Anthonisen N.R., et. al.: C-reactive protein and mortality in mild to moderate chronic obstructive pulmonary disease. Thorax 2006; 61: pp. 849-853.
7. Anthonisen N.R., Connett J.E., Enright P.L., et. al., Lung Health Study Research Group: Hospitalizations and mortality in the Lung Health Study. Am J Respir Crit Care Med 2002; 166: pp. 333-339.
8. Calverley P.M., Anderson J.A., Celli B., et. al.: TORCH investigators. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med 2007; 356: pp. 775-789.
9. Ross R.: The pathogenesis of atherosclerosis: a perspective for the 1990s. Nature 1993; 362: pp. 801-809.
10. Faxon D.P., Fuster V., Libby P., et. al.: Atherosclerotic vascular disease conference: writing group iii: pathophysiology. Circulation 2004; 109: pp. 2617-2625.
11. Ross R.: Atherosclerosis – an inflammatory disease. N Engl J Med 1999; 340: pp. 115-126.
12. Bonetti P.O., Lerman L.O., Lerman A.: Endothelial dysfunction: a marker of atherosclerotic risk. Arterioscler Thromb Vasc Biol 2003; 23: pp. 168-175.
13. Anderson T.J., Uehata A., Gerhard M.D., et. al.: Close relation of endothelial function in the human coronary and peripheral circulations. J Am Coll Cardiol 1995; 26: pp. 1235-1241.
14. Neunteufl T., Katzenschlager R., Hassan A., et. al.: Systemic endothelial dysfunction is related to the extent and severity of coronary artery disease. Atherosclerosis 1997; 129: pp. 111-118.
15. Barr R.G., Mesia-Vela S., Austin J.H., et. al.: Impaired flow-mediated dilation is associated with low pulmonary function and emphysema in ex-smokers: the Emphysema and Cancer Action Project (EMCAP) Study. Am J Respir Crit Care Med 2007; 176: pp. 1200-1207.
16. McAllister D.A., Maclay J.D., Mills N.L., et. al.: Arterial stiffness is independently associated with emphysema severity in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2007; 176: pp. 1208-1214.
17. Mills N.L., Miller J.J., Anand A., et. al.: Increased arterial stiffness in patients with chronic obstructive pulmonary disease: a mechanism for increased cardiovascular risk. Thorax 2008; 63: pp. 306-311.
18. Eickhoff P., Valipour A., Kiss D., et. al.: Determinants of systemic vascular function in patients with stable chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2008; 178: pp. 1211-1218.
19. Iwamoto H., Yokoyama A., Kitahara Y., et. al.: Airflow limitation in smokers is associated with subclinical atherosclerosis. Am J Respir Crit Care Med 2009; 179: pp. 35-40.
20. Sabit R., Bolton C.E., Edwards P.H., et. al.: Arterial stiffness and osteoporosis in chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2007; 175: pp. 1259-1265.
21. Bostrom K., Watson K.E., Horn S., et. al.: Bone morphogenetic protein expression in human atherosclerotic lesions. J Clin Invest 1993; 91: pp. 1800-1809.
22. Shanahan C.M., Cary N.R., Metcalfe J.C., et. al.: High expression of genes for calcification-regulating proteins in human atherosclerotic plaque. J Clin Invest 1994; 93: pp. 2393-2402.
23. Witteman J.C., Kannel W.B., Wolf P.A., et. al.: Aortic calcified plaques and cardiovascular disease (the Framingham Study). Am J Cardiol 1990; 66: pp. 1060-1064.
24. Takasu J., Katz R., Nasir K., et. al.: Relationships of thoracic aortic wall calcification to cardiovascular risk factors: the Multi-Ethnic Study of Atherosclerosis (MESA). Am Heart J 2008; 155: pp. 765-771.
25. Eisen A., Tenenbaum A., Koren-Morag N., et. al.: Calcification of the thoracic aorta as detected by spiral computed tomography among stable angina pectoris patients: association with cardiovascular events and death. Circulation 2008; 118: pp. 1328-1334.
26. Takasu J., Mao S., Budoff M.J.: Aortic atherosclerosis detected with electron-beam CT as a predictor of obstructive coronary artery disease. Acad Radiol 2003; 10: pp. 631-637.
27. Takasu J., Katz R., Shavelle D.M., et. al.: Inflammation and descending thoracic aortic calcification as detected by computed tomography: the Multi-Ethnic Study of Atherosclerosis. Atherosclerosis 2008; 199: pp. 201-206.
28. Kasahara Y., Tuder R.M., Taraseviciene-Stewart L., et. al.: Inhibition of VEGF receptors causes lung cell apoptosis and emphysema. J Clin Invest 2000; 106: pp. 1311-1319.
29. Santos S., Peinado V.I., Ramirez J., et. al.: Enhanced expression of vascular endothelial growth factor in pulmonary arteries of smokers and patients with moderate chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2003; 167: pp. 1250-1256.
30. Peinado V.I., Barberá J.A., Abate P., et. al.: Inflammatory reaction in pulmonary muscular arteries of patients with mild chronic obstructive pulmonary disease. Am J Respir Crit Care Med 1999; 159: pp. 1605-1611.
31. Matsuoka S., Washko G.R., Dransfield M.T., et. al.: Quantitative CT measurement of cross-sectional area of small pulmonary vessel in COPD: correlations with emphysema and airflow limitation. Acad Radiol 2010; 17: pp. 93-99.
32. Matsuoka S., Washko G.R., Yamashiro T., et. al., National Emphysema Treatment Trial Research Group: Pulmonary hypertension and CT measurement of small pulmonary vessels in severe emphysema. Am J Respir Crit Care Med 2010; 181: pp. 218-225.
33. Miller M.R., Hankinson J., Brusasco V., et. al.: Standardisation of spirometry. Eur Respir J 2005; 26: pp. 319-338.
34. Coche E., Pawlak S., Dechambre S., et. al.: Peripheral pulmonary arteries: identification at multi-slice spiral CT with 3D reconstruction. Eur Radiol 2003; 13: pp. 815-822.
35. Shemesh J., Apter S., Rozenman J., et. al.: Calcification of coronary arteries: detection and quantification with double-helix CT. Radiology 1995; 197: pp. 779-783.
36. Agaston A.S., Janowitz W.R., Hildner F.J., et. al.: Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol 1990; 15: pp. 827-832.
37. Eisen A., Tenenbaum A., Koren-Morag N., et. al.: Calcification of the thoracic aorta as detected by spiral computed tomography among stable angina pectoris patients: association with cardiovascular events and death. Circulation 2008; 118: pp. 1328-1334.
38. Wu M.H., Chern M.S., Chen L.C., et. al.: Electron beam computed tomography evidence of aortic calcification as an independent determinant of coronary artery calcification. J Chin Med Assoc 2006; 69: pp. 409-414.
39. Gevenois P.A., de Maertelaer V., De Vuyst P., et. al.: Comparison of computed density and macroscopic morphometry in pulmonary emphysema. Am J Respir Crit Care Med 1995; 152: pp. 653-657.
40. Chaouat A., Savale L., Chouaid C., et. al.: Role for interleukin-6 in COPD-related pulmonary hypertension. Chest 2009; 136: pp. 678-687.
41. Maclay J.D., McAllister D.A., Mills N.L., et. al.: Vascular dysfunction in chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2009; 180: pp. 513-520.
42. Schünemann H.J., Dorn J., Grant B.J., et. al.: Pulmonary function is a long-term predictor of mortality in the general population: 29-year follow-up of the Buffalo Health Study. Chest 2000; 118: pp. 656-664.
43. Bang K.M., Gergen P.J., Kramer R., et. al.: The effect of pulmonary impairment on all-cause mortality in a national cohort. Chest 1993; 103: pp. 536-540.
44. Friedman G.D., Klatsky A.L., Siegelaub A.B.: Lung function and risk of myocardial infarction and sudden cardiac death. N Engl J Med 1976; 294: pp. 1071-1075.
45. Hale K.A., Niewoehner D.E., Cosio M.G.: Morphologic changes in the muscular pulmonary arteries: relationship to cigarette smoking, airway disease, and emphysema. Am Rev Respir Dis 1980; 122: pp. 273-278.
46. Wright J.L., Lawson L., Pare P.D., et. al.: The structure and function of the pulmonary vasculature in mild chronic obstructive pulmonary disease. The effect of oxygen and exercise. Am Rev Respir Dis 1983; 128: pp. 702-707.
47. Santos S., Peinado V.I., Ramirez J., et. al.: Characterization of pulmonary vascular remodelling in smokers and patients with mild COPD. Eur Respir J 2002; 19: pp. 632-638.
48. Kasahara Y., Tuder R.M., Cool C.D., et. al.: Endothelial cell death and decreased expression of vascular endothelial growth factor and vascular endothelial growth factor receptor 2 in emphysema. Am J Respir Crit Care Med 2001; 163: pp. 737-744.
49. Kanazawa H., Asai K., Hirata K., Yoshikawa J.: Possible effects of vascular endothelial growth factor in the pathogenesis of chronic obstructive pulmonary disease. Am J Med 2003; 114: pp. 354-358.
50. Schroeder E.B., Welch V.L., Evans G.W., et. al.: Impaired lung function and subclinical atherosclerosis. The ARIC Study. Atherosclerosis 2005; 180: pp. 367-373.