
Rationale and Objectives
Present methods for measuring adherence to national imaging quality measures often require a resource-intensive chart review. Computerized decision support systems may allow for automated capture of these data. We sought to determine the feasibility of measuring adherence to a national quality measure (NQM) regarding computed tomography pulmonary angiograms (CTPAs) for pulmonary embolism using measure-targeted clinical decision support and whether the associated increased burden of data captured required by this system would affect the use and yield of CTs.
Materials and Methods
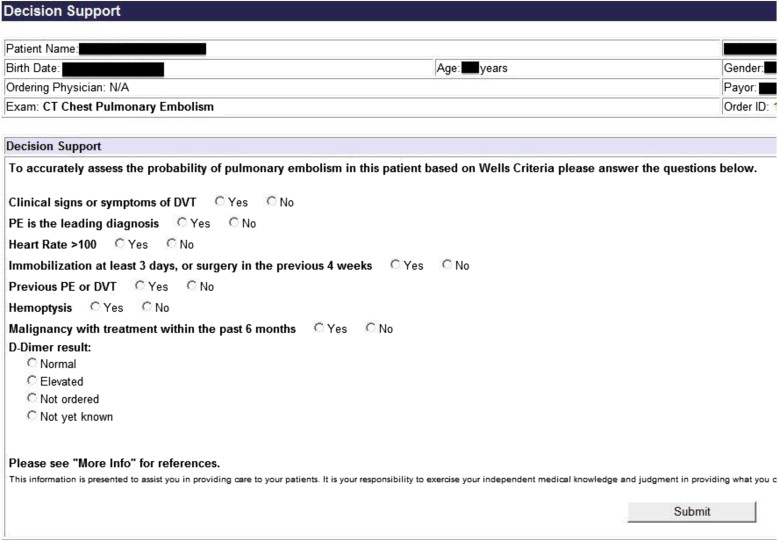
This institutional review board–approved prospective cohort study enrolled patients from September 1, 2009, through November 30, 2011, in the emergency department (ED) of a 776-bed quaternary-care adults-only academic medical center. Our intervention consisted of an NQM-targeted clinical decision support tool for CTPAs, which required mandatory input of the Wells criteria and serum D-dimer level. The primary outcome was the documented adherence to the quality measure prior and subsequent to the intervention, and the secondary outcomes were the use and yield of CTPAs.
Results
A total of 1209 patients with suspected PE (2.0% of 58,795 ED visits) were imaged by CTPA during the 12-month control period, and 1212 patients were imaged in the 12 months after the quarter during which the intervention was implemented (2.0% of 59,478 ED visits, P = .84). Documented baseline adherence to the NQM was 56.9% based on a structured review of the provider notes. After implementation, documented adherence increased to 75.6% ( P < .01). CTPA yield remained unchanged and was 10.4% during the control period and 10.1% after the intervention ( P = .88).
Conclusions
Implementation of a clinical decision support tool significantly improved documented adherence to an NQM, enabling automated measurement of provider adherence to evidence without the need for resource-intensive chart review. It did not adversely affect the use or yield of CTPAs.
Present health care reform initiatives focus on increasing value, improving quality, and reducing waste, often through the use of publicly reported national quality measures (NQMs) . Much of this activity has been directed toward the use of high-cost imaging such as computed tomography (CT), the use of which has increased significantly over the past two decades . Although CT is useful because of its diagnostic speed and accuracy , it has come under scrutiny because of its potential for inappropriate use, especially in the emergency department (ED) , and its potential risks of radiation exposure and contrast-induced nephropathy .
One area of intense focus is the ED use of CT for patients with suspected pulmonary embolism (PE). Although validated, evidence-based decision tools designed to help clinicians to identify patients who need imaging have been available for more than 12 years and are now endorsed by multiple specialty societies , inappropriate use continues, and educational interventions have not been shown to improve appropriateness . An evidence-based NQM was recently endorsed by the National Quality Forum but, in a recent study, one-third of the CT pulmonary angiograms (CTPAs) performed in ED patients with suspected PE did not adhere to it . Another recent study demonstrated that pretest probabilities are rarely documented by emergency physicians before obtaining CTPAs . Additionally, a number of public comments regarding the NQM cited concerns regarding the level of intensive manual chart review that would be necessary to gather the granular data required to determine whether CTPAs were adherent to evidence .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Study Design and Setting
Get Radiology Tree app to read full this article<
Study Participants
Get Radiology Tree app to read full this article<
Intervention
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Sample Size
Get Radiology Tree app to read full this article<
Data Collection
Get Radiology Tree app to read full this article<
Statistical Analyses
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Comparison of Control and Intervention Patient Cohorts
Control Period Intervention Period_P_ Value Age, y (SD) 56.0 (16.9) 55.1 (17.0) .81 Male 36.7% 38.4% .70 Use of CTPA, % of all ED visits 2.1% 2.0% .84 NQM adherence 56.9% 75.6%0.008 CTPA yield 10.4% 10.1% .88
CTPA, computed tomography pulmonary angiography; ED, emergency department; NQM, national quality measure; SD, standard deviation.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Iglehart J.K.: The new era of medical imaging—progress and pitfalls. N Engl J Med 2006; 354: pp. 2822-2828.
2. Lamb G.C., Smith M.A., Weeks W.B., et. al.: Publicly reported quality-of-care measures influenced Wisconsin physician groups to improve performance. Health Aff 2013; 32: pp. 536-543.
3. Spinks T.E., Walters R., Feeley T.W., et. al.: Improving cancer care through public reporting of meaningful quality measures. Health Aff 2011; 30: pp. 664-672.
4. Broder J., Warshauer D.M.: Increasing utilization of computed tomography in the adult emergency department, 2000–2005. Emerg Radiol 2006; 13: pp. 25-30.
5. Lee J., Kirschner J., Pawa S., et. al.: Computed tomography use in the adult emergency department of an academic urban hospital from 2001 to 2007. Ann Emerg Med 2010; Available at: http://www.annemergmed.com/article/S0196-0644(10)00499-3/abstract Accessed October 12, 2010
6. Raja A.S., Wright C., Sodickson A.D., et. al.: Negative appendectomy rate in the era of CT: an 18-year perspective. Radiology 2010; 256: pp. 460-465.
7. Fesmire F.M., Brown M.D., Espinosa J.A., et. al.: Critical issues in the evaluation and management of adult patients presenting to the emergency department with suspected pulmonary embolism. Ann Emerg Med 2011; 57: pp. 628-652.e75.
8. Corwin M.T., Donohoo J.H., Partridge R., et. al.: Do emergency physicians use serum D-dimer effectively to determine the need for CT when evaluating patients for pulmonary embolism? Review of 5,344 consecutive patients. AJR Am J Roentgenol 2009; 192: pp. 1319-1323.
9. Brenner D.J., Hall E.J.: Computed tomography—an increasing source of radiation exposure. N Engl J Med 2007; 357: pp. 2277-2284.
10. Mitchell A.M., Jones A.E., Tumlin J.A., et. al.: Prospective study of the incidence of contrast-induced nephropathy among patients evaluated for pulmonary embolism by contrast-enhanced computed tomography. Acad Emerg Med 2012; 19: pp. 618-625.
11. Wells P.S., Anderson D.R., Rodger M., et. al.: Derivation of a simple clinical model to categorize patients probability of pulmonary embolism: increasing the models utility with the SimpliRED D-dimer. Thromb Haemost 2000; 83: pp. 416-420.
12. Segal J.B., Eng J., Tamariz L.J., et. al.: Review of the evidence on diagnosis of deep venous thrombosis and pulmonary embolism. Ann Fam Med 2007; 5: pp. 63-73.
13. Torbicki A., Perrier A., Konstantinides S., et. al.: Guidelines on the diagnosis and management of acute pulmonary embolism: the Task Force for the Diagnosis and Management of Acute Pulmonary Embolism of the European Society of Cardiology (ESC). Eur Heart J 2008; 29: pp. 2276-2315.
14. Costantino M.M., Randall G., Gosselin M., et. al.: CT angiography in the evaluation of acute pulmonary embolus. AJR Am J Roentgenol 2008; 191: pp. 471-474.
15. Teismann N.A., Cheung P.T., Frazee B.: Is the ordering of imaging for suspected venous thromboembolism consistent with D-dimer result?. Ann Emerg Med 2009; 54: pp. 442-446.
16. Venkatesh A., Kline J., Courtney M., et. al.: Evaluation of ulmonary embolism in the emergency department and consistency with a national quality measure. Arch Intern Med 2012; 1:
17. Crichlow A., Cuker A., Mills A.M.: Overuse of computed tomography pulmonary angiography in the evaluation of patients with suspected pulmonary embolism in the emergency department. Acad Emerg Med 2012; 19: pp. 1219-1226.
18. Prasad V., Rho J., Cifu A.: The diagnosis and treatment of pulmonary embolism: a metaphor for medicine in the evidence-based medicine era. Arch Intern Med 2012; 172: pp. 955-958.
19. Kanaan Y., Knoepp U.D., Kelly A.M.: The influence of education on appropriateness rates for CT pulmonary angiography in emergency department patients. Acad Radiol 2013; 20: pp. 1107-1114.
20. NQF: National Voluntary Consensus Standards for imaging efficiency: a consensus report. Available at: http://www.qualityforum.org/Publications/2012/01/National_Voluntary_Consensus_Standards_for_Imaging_Efficiency__A_Consensus_Report.aspx , Accepted. January 25, 2013.
21. Hedner C., Sundgren P.C., Kelly A.M.: Associations between presence of relevant information in referrals to radiology and prevalence rates in patients with suspected pulmonary embolism. Acad Radiol 2013 Sep; 20: pp. 1115-1121.
22. Khorasani R.: Computerized physician order entry and decision support: improving the quality of care. Radiographics 2001 Aug; 21: pp. 1015-1018.
23. Romano M.J., Stafford R.S.: Electronic health records and clinical decision support systems: impact on national ambulatory care quality. Arch Intern Med 2011 May 23; 171: pp. 897-903.
24. Blumenthal D.: Launching HITECH. N Engl J Med 2010 Feb 4; 362: pp. 382-385.
25. Khorasani R., Menard A.: Qualifying for incentive payments for meaningful use of health care IT for radiologists: practical initial steps. J Am Coll Radiol 2011 Apr; 8: pp. 222-224.
26. Conway P.H., Mostashari F., Clancy C.: The future of quality measurement for improvement and accountability. JAMA 2013 Jun 5; 309: pp. 2215-2216.
27. Raja A.S., Ip I.K., Prevedello L.M., et. al.: Effect of computerized clinical decision support on the use and yield of CT pulmonary angiography in the emergency department. Radiology 2012 Feb 1; 262: pp. 468-474.
28. Ip I.K., Schneider L.I., Hanson R., et. al.: Adoption and meaningful use of computerized physician order entry with an integrated clinical decision support system for radiology: ten-year analysis in an urban teaching hospital. J Am Coll Radiol 2012 Feb; 9: pp. 129-136.
29. Prevedello LM, Raja AS, Ip IK, et al. Effect of clinical decision support on intra- and inter-physician variation in the yield of CT in patients with suspected pulmonary embolism. In Press.
30. Garg A.X., Adhikari N.K.J., McDonald H., et. al.: Effects of computerized clinical decision support systems on practitioner performance and patient outcomes. JAMA 2005 Mar 9; 293: pp. 1223-1238.
31. Blackmore C.C., Mecklenburg R.S., Kaplan G.S.: Effectiveness of clinical decision support in controlling inappropriate imaging. J Am Coll Radiol 2011 Jan; 8: pp. 19-25.
32. Rosenthal D.I., Weilburg J.B., Schultz T., et. al.: Radiology order entry with decision support: initial clinical experience. J Am Coll Radiol 2006 Oct; 3: pp. 799-806.
33. Bowen S., Johnson K., Reed M.H., et. al.: The effect of incorporating guidelines into a computerized order entry system for diagnostic imaging. J Am Coll Radiol 2011 Apr; 8: pp. 251-258.