
Rationale and Objectives
Lung cancer is the leading cause of cancer death in the United States. Mortality outcomes have improved only modestly over the past 30 years. There is intense focus on the development of better treatments for lung cancer. Major issues include the cost and time duration of the clinical trials required to establish the utility of a drug so that it can be formally approved by regulatory agencies. In clinical settings, biomarkers that accelerate assessments of responses to treatment could benefit patients by providing earlier diagnoses of progressive disease, particularly when there are multiple options for treatment, and the effects of toxicity from one treatment tend to limit the ability to administer the next line of therapy.
Materials and Methods
Quantifying longitudinal changes in tumor volumes using computed tomography could eventually become a more useful surrogate endpoint for assessing tumor responses or progression events than simple unidimensional measurements.
Results
The authors review the historical development of response measurements in lung cancer, set out the medical context for specifying volumetric imaging requirements and goals, compare volumetric technique to conventional methods, and identify the imaging profiles being pursued.
Conclusion
The Quantitative Imaging Biomarkers Alliance is investigating volumetric computed tomographic acquisition and analytic methods to increase the analytic power per subject enrolled in clinical trials to reduce the number of total subjects needed or shorten the length of time an individual needs to be followed to reliably establish drug response.
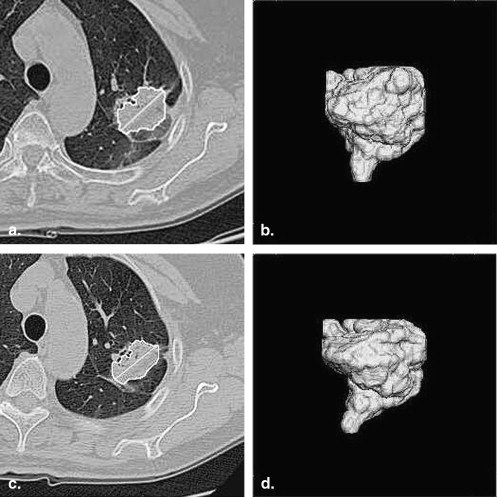
Computed tomographic imaging technology has continued to improve over the past three decades . The benefits of imaging for diagnosis, staging, and restaging cancer are now well established . However, assessing responses to treatment has remained predominantly qualitative, with limited use of electronic caliper measurements of unidimensional or bidimensional line lengths on a single two-dimensional image slice. Anecdotal evidence continues to emerge suggesting that line-length measurements may be misleading compared to volumetric measurements of the tumor mass. However, early attempts to quantify entire tumor volumes proved to be labor intensive and not adequately reproducible . More recent attempts have been encouraging , but additional studies are needed for future consideration as an acceptable imaging endpoint by regulatory authorities.
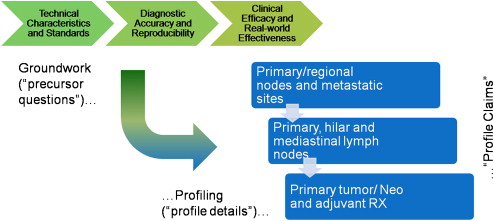
This report outlines the initial clinical emphasis of the Volumetric CT Technical Committee of the Radiological Society of North America’s (RSNA) Quantitative Imaging Biomarkers Alliance (QIBA). The potential benefits of the effort are described, the roles of each of the stakeholders are explained, and a staged approach for moving the process forward is explained.
Opportunity
Get Radiology Tree app to read full this article<
Historical development of response measurements in lung cancer
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
The medical context for volumetric imaging
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Cancer staging
Get Radiology Tree app to read full this article<
Table 1
Summary of Image-processing Issues Relative to Stages of Lung Cancer
Stage % of Cases % 5-year Survival Imaging Focus/Therapy Focus Imaging Tool Issues Thoracic Segmentation High-resolution Techniques I 16 49 Primary tumor/neoadjuvant and adjuvant therapy sCT Small cancers surrounded by air Can be straightforward Needed II/III 35 15.2 Primary, hilar and mediastinal lymph nodes/combined modality sCT, PET Larger tumors and nodes abut other structures Often challenging Optional IV 41 3 Primary/regional nodes and metastatic sites/chemotherapy sCT, PET, bone, brain scans Tumor response often determined outside of the chest Often challenging Optional
PET, positron emission tomography; sCT, spiral computed tomography.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Volumetric technique versus conventional methods: preliminary clinical studies in non-small-cell lung cancer
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Lung cancer profiles
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Next steps
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
References
1. Fuchs T., Kachelrieß M., Kalender W.A.: Technical advances in multi-slice spiral CT. Eur J Radiol 2000; 36: pp. 69-73.
2. Tempany C.M.C., McNeil B.J.: Advances in biomedical imaging. JAMA 2001; 285: pp. 562-567.
3. Diederich S., Wormanns D.: Impact of low-dose CT on lung cancer screening. Lung Cancer 2004; 45: pp. S13-S19.
4. Wang Y., van Klaveren R.J., van der Zaag-Loonen H.J., et. al.: Effect of nodule characteristics on variability of semiautomated volume measurements in pulmonary nodules detected in a lung cancer screening program. Radiology 2008; 248: pp. 625-631.
5. Das M., Ley-Zaporozhan J., Gietema H.A.: Accuracy of automated volumetry of pulmonary nodules across different multislice CT scanners. Eur Radiol 2007; 17: pp. 1979-1984.
6. Jemal A., Siegel R., Ward E., et. al.: Cancer statistics, 2008. CA Cancer J Clin 2008; pp. 71-96.
7. Wakelee H.A., Bernardo P., Johnson D.H., Schiller J.H.: Changes in the natural history of nonsmall cell lung cancer (NSCLC)—comparison of outcomes and characteristics in patients with advanced NSCLC entered in Eastern Cooperative Oncology Group trials before and after 1990. Cancer 2006; 106: pp. 2208-2217.
8. Mayburd A.L., Golovchikova I., Mulshine J.L.: Successful anti-cancer drug targets able to pass FDA review demonstrate the identifiable signature distinct from the signatures of random genes and initially proposed targets. Bioinformatics 2008; 24: pp. 389-395.
9. World Health Organization : WHO handbook for reporting results of cancer treatment.1979.World Health OrganizationGeneva, Switzerland
10. Miller A.B., Hogestraeten B., Staquet M., et. al.: Reporting results of cancer treatment. Cancer 1981; 47: pp. 207-214.
11. Therasse P., Arbuck S.G., Eisenhauer E.A., et. al.: New guidelines to evaluate response to treatment in solid tumors. J Natl Cancer Inst 2000; 92: pp. 205-216.
12. Eisenhauer E.A., Therasse P., Bogaerts J., et. al.: New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer 2009; 45: pp. 228-247.
13. Sohaib S.A., Turner B., Hanson J.A., et. al.: CT assessment of tumour response to treatment: comparison of linear, cross-sectional and volumetric measures of tumours size. Br J Radiol 2000; 73: pp. 1178-1184.
14. Warren K.E., Patronas N., Aikin A.A., Albert P.S., Balis F.M.: Comparison of one-, two-, and three-dimensional measurements of childhood brain tumors. J Natl Cancer Inst 2001; 93: pp. 1401-1405.
15. Trillet-Lenoir V., Freyer G., Kaemmerlenet P., et. al.: Assessment of tumour response to chemotherapy for metastatic colorectal cancer: accuracy of the RECIST criteria. Br J Radiol 2002; 75: pp. 903-908.
16. Schwartz L.H., Mazumdar M., Wang L., et. al.: Response assessment classification in patients with advanced renal cell carcinoma treated on clinical trials. Cancer 2003; 98: pp. 1611-1619.
17. McHugh K., Kao S.: Can paediatric radiologists resist RECIST (response evaluation criteria in solid tumours)?. Pediatr Radiol 2003; 33: pp. 739-743.
18. Moertel C.G., Hanley J.A.: The effect of measuring error on the results of therapeutic trials in advanced cancer. Cancer 1976; 38: pp. 388-394.
19. Lavin P.T., Flowerdew G.: Studies in variation associated with the measurement of solid tumors. Cancer 1980; 46: pp. 1286-1290.
20. Gandara D.R., Aberle D., Lau D., et. al.: Radiographic imaging of bronchioloalveolar carcinoma: screening, patterns of presentation and response assessment. J Thorac Oncol 2006; 1: pp. S20-S26.
21. Goldstraw P., Crowley J., Chansky K., et. al.: The IASLC Lung Cancer Staging Project: proposals for the revision of the TNM stage groupings in the forthcoming (seventh) edition of the TNM classification of malignant tumours. J Thorac Oncol 2007; 2: pp. 706-714.
22. Wakelee H., Chhatwani L.: Adjuvant chemotherapy for resected non-small cell lung cancer. Semin Thorac Cardiovasc Surg 2008; 20: pp. 198-203.
23. Mulshine J.L.: Early lung cancer detection: approaching the “tipping point”. Oncology (Williston Park) 2006; 20: pp. 1632.
24. Stoel B.C., Putter H., Bakker M.E., et. al.: Volume correction in computed tomography densitometry for follow-up studies on pulmonary emphysema. Proc Am Thorac Soc 2008; 5: pp. 919-924.
25. Zhao B., Schwartz L.H., Moskowitz C., Ginsberg M.S., Rizvi N.A., Kris M.G.: Computerized quantification of tumor response in lung cancer—initial results. Radiology 2006; 241: pp. 892-898.
26. Zhao B., James L., Moskowitz C., et. al.: Evaluating variability in tumor measurements from same-day repeat CT scans in patients with non-small cell lung cancer. Radiology 2009; 252: pp. 263-272.
27. Revel M.-P., Bissery A., Bienvenu M., Aycard L., Lefort C., Frija G.: Are two-dimensional CT measurements of small noncalcified pulmonary nodules reliable?. Radiology 2004; 231: pp. 453-458.
28. Buckler AJ, et al. Volumetric CT in lung cancer: an example for the qualification of imaging as a biomarker. Acad Radiol. In press.
29. Volumetric CT. Available at: http://qibawiki.rsna.org/index.php?title=Volumetric_CT . Accessed October 27, 2009.