
Rationale and Objectives
To determine if focal liver masses could be differentiated as benign or malignant on the basis of diffusion-weighted imaging (DWI).
Methods and Materials
A total of 104 patients with focal liver masses were scanned using 1.5 T magnetic resonance imaging (MRI). DWI was performed with b values of 0, 50, and 400 s/mm 2 . Of these, 76 patients had lesions larger than 2 cm diameter, radiologic or pathologic characterization of the lesion, and diagnostic quality DWI. The apparent diffusion coefficient (ADC) of the largest liver lesion was measured. The liver masses were diagnosed on histology or had characteristic computed tomography/MRI findings and follow up of more than 6 months. The analyzed lesions were hemangioma ( n = 17), cysts ( n = 5), hepatocellular cancer (HCC) ( n = 41), adenoma ( n = 3), focal nodular hyperplasia (FNH) ( n = 6), and metastases ( n = 4).
Results
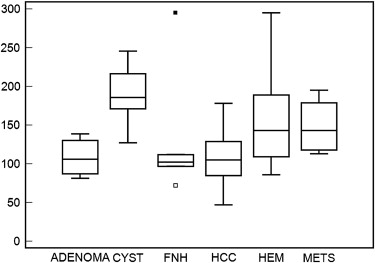
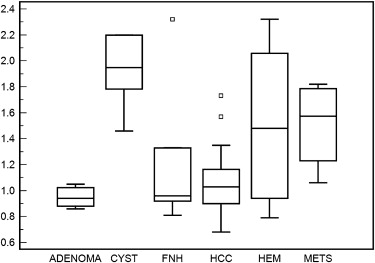
The mean (standard deviation) ADC values (10 −5 mm 2 /second) of hemangiomas, cysts, FNH, and HCC were 156.8 (54.1), 190.2 (43.0), 130.1 (81.9), and 107.6 (32.7). The ADC of cysts and hemangiomas were significantly higher than that of other lesions ( P = .0003, t -test). There was no significant difference between ADC values of solid, benign liver lesions (FNH, adenoma) and malignant lesions (HCC, metastases) ( P = .62).
Conclusion
Solid liver lesions have a lower ADC than cysts and hemangiomas. However, there is no significant difference in ADC between solid benign and malignant lesions. DWI appears to have only minimal additional value over currently used MRI sequences in characterizing liver masses.
With the increasing use of computed tomography (CT) and magnetic resonance imaging (MRI), incidental liver lesions are increasingly identified. Even in patients undergoing staging for known malignancy, liver lesions may be identified that cannot be characterized with reasonable certainty. The ability to definitely diagnose liver lesions has many clinical benefits, including obviating the need for invasive techniques such as biopsy or resection surgery. An indeterminate diagnosis often requires follow-up imaging in several months, and may result in considerable anxiety to the patient and cost to the health system. In the last few years, progress has been made in imaging characterization of liver lesions. Delayed scanning with gadobenate dimeglumine (MultiHance, Bracco Diagnostics, Princeton, NJ) has been reported to help in differentiating focal nodular hyperplasia from other hypervascular lesions, including hepatic adenomas . Studies have indicated the usefulness of MRI studies performed using protocols involving two contrast agents, superparamagnetic iron oxide particles and conventional gadolinium, in improving accuracy for hepatocellular carcinoma in cirrhotic patients . Microbubble-enhanced sonography is being evaluated for its use in characterizing liver lesions .
Diffusion is the random, thermally induced movement of water molecules. Diffusion of intracellular water molecules is reduced due to the presence of the membranes that encase the cell and its organelles. Conversely, diffusion is less restricted in the normal extracellular space. In general, malignant lesions are more cellular than benign lesions. Therefore, diffusion would be expected to be lower in malignant than in benign lesions, and diffusion-weighted MRI (DWI) potentially may be a robust method for differentiating malignant and benign lesions. In this study, we investigated whether DWI can help differentiate benign from malignant liver lesions.
Methods
Patients
Get Radiology Tree app to read full this article<
MRI Examination
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Confirmation of Liver Lesions
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Lesion Characteristics
Get Radiology Tree app to read full this article<
Interobserver Correlation
Get Radiology Tree app to read full this article<
ADC Values of Lesions
Get Radiology Tree app to read full this article<
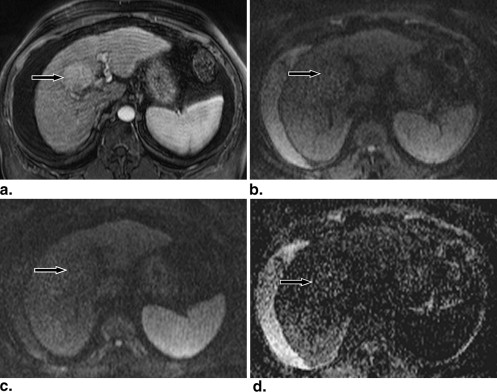
![Figure 2, A 61-year-old male on follow-up 7 years after orthotopic liver transplantation. (a) T2-weighted magnetic resonance imaging (MRI) sequence (repetition time/echo time [TR/TE] [ms], flip angle, echo train length: 5301/104, 150, 13) shows very high signal lesion in lateral right lobe (arrow) . (b) There is no contrast enhancement in the lesion (arrow) on three-dimensional T1-weighted image (TR/TE [ms], flip angle: 4.85/2.48, 12°) after 20 mL of gadobenate dimeglumine (MultiHance, Bracco Diagnostics, Princeton, NJ). The lesion is radiologically diagnosed as a cyst. (c) ADC map shows the lesion to be very bright. The mean ADC value is 234 × 10 −5 mm 2second.](https://storage.googleapis.com/dl.dentistrykey.com/clinical/TheValueofDiffusionWeightedImaginginCharacterizingFocalLiverMasses/1_1s20S1076633209003122.jpg)
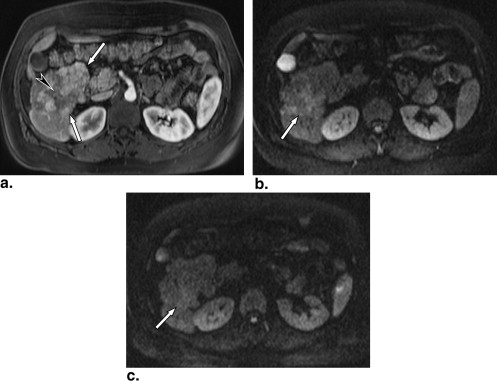
![Figure 3, A 27-year-old female had a magnetic resonance imaging scan to characterize a low-density lesion seen on computed tomography. (a,b) T1-weighted sequence (repetition time/echo time [TR/TE] (ms), flip angle: 4.85/2.48, 12°) obtained in arterial (a) and venous (b) phases after 17 mL of gadobenate dimeglumine shows progressive puddling of contrast within the lesion (arrow) consistent with a hemangioma. (c,d) Diffusion-weighted images performed with b value of 50 (c) and 400 (d) s/mm 2 show that the lesion (arrows) has high signal on both sequences. (e) Apparent diffusion coefficient (ADC) maps also indicates high signal within the lesion. The ADC value was measured at 205 × 10 −5 mm 2second.](https://storage.googleapis.com/dl.dentistrykey.com/clinical/TheValueofDiffusionWeightedImaginginCharacterizingFocalLiverMasses/2_1s20S1076633209003122.jpg)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
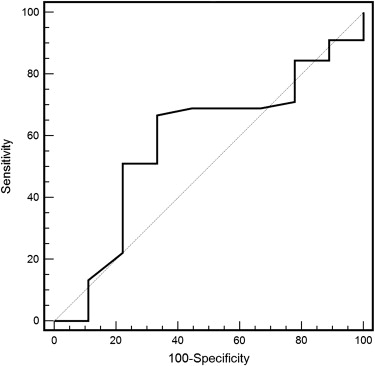
Prediction of Benignity vs. Malignancy using ADC and ADC Lesion-to-liver Ratios
AUC Best Value Sensitivity (%) Specificity (%) ADC 0.50 104 ∗ 54 44 ADC liver-to-lesion ratio 0.58 1.0 0.67 0.67
ADC, apparent diffusion coefficient.
The table gives the area under the receiver operating characteristic curve (AUC) and the value of ADC or ADC lesion-to-liver ratio that is associated with maximized sensitivity and specificity for differentiating solid benign lesions from malignant lesions.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Grazioli L., Morana G., Kirchin M.A., et. al.: Accurate differentiation of focal nodular hyperplasia from hepatic adenoma at gadobenate dimeglumine-enhanced MR imaging: prospective study. Radiology 2005; 236: pp. 166-177.
2. Grazioli L., Morana G., Federle M.P., et. al.: Focal nodular hyperplasia: morphologic and functional information from MR imaging with gadobenate dimeglumine. Radiology 2001; 221: pp. 731-739.
3. Hanna R.F., Kased N., Kwan S.W., et. al.: Double-contrast MRI for accurate staging of hepatocellular carcinoma in patients with cirrhosis. AJR Am J Roentgenol 2008; 190: pp. 47-57.
4. Macarini L., Marini S., Milillo P., et. al.: Double-contrast MRI (DC-MRI) in the study of the cirrhotic liver: utility of administering Gd-DTPA as a complement to examinations in which SPIO liver uptake and distribution alterations (SPIO-LUDA) are present and in the identification and characterisation of focal lesions. Radiol Med (Torino) 2006; 111: pp. 1087-1102.
5. Burns P.N., Wilson S.R.: Focal liver masses: enhancement patterns on contrast-enhanced images–concordance of US scans with CT scans and MR images. Radiology 2007; 242: pp. 162-174.
6. Larsen L.P., Rosenkilde M., Christensen H., et. al.: The value of contrast enhanced ultrasonography in detection of liver metastases from colorectal cancer: a prospective double-blinded study. Eur J Radiol 2007; 62: pp. 302-307.
7. Wang J.H., Lu S.N., Hung C.H., et. al.: Small hepatic nodules (< or =2 cm) in cirrhosis patients: characterization with contrast-enhanced ultrasonography. Liver Int 2006; 26: pp. 928-934.
8. Lewin M., Poujol-Robert A., Boelle P.Y., et. al.: Diffusion-weighted magnetic resonance imaging for the assessment of fibrosis in chronic hepatitis C. Hepatology 2007; 46: pp. 658-665.
9. Taouli B., Tolia A.J., Losada M., et. al.: Diffusion-weighted MRI for quantification of liver fibrosis: preliminary experience. AJR Am J Roentgenol 2007; 189: pp. 799-806.
10. Koh D.M., Collins D.J.: Diffusion-weighted MRI in the body: applications and challenges in oncology. AJR Am J Roentgenol 2007; 188: pp. 1622-1635.
11. Le B.D., Breton E., Lallemand D., et. al.: Separation of diffusion and perfusion in intravoxel incoherent motion MR imaging. Radiology 1988; 168: pp. 497-505.
12. Naganawa S., Kawai H., Fukatsu H., et. al.: Diffusion-weighted imaging of the liver: technical challenges and prospects for the future. Magn Reson Med Sci 2005; 4: pp. 175-186.
13. Moteki T., Horikoshi H., Oya N., et. al.: Evaluation of hepatic lesions and hepatic parenchyma using diffusion-weighted reordered turboFLASH magnetic resonance images. J Magn Reson Imaging 2002; 15: pp. 564-572.
14. Namimoto T., Yamashita Y., Sumi S., et. al.: Focal liver masses: characterization with diffusion-weighted echo-planar MR imaging. Radiology 1997; 204: pp. 739-744.
15. Quan X.Y., Sun X.J., Yu Z.J., et. al.: Evaluation of diffusion weighted imaging of magnetic resonance imaging in small focal hepatic lesions: a quantitative study in 56 cases. Hepatobiliary Pancreat Dis Int 2005; 4: pp. 406-409.
16. Sun X.J., Quan X.Y., Huang F.H., et. al.: Quantitative evaluation of diffusion-weighted magnetic resonance imaging of focal hepatic lesions. World J Gastroenterol 2005; 11: pp. 6535-6537.
17. Taouli B., Vilgrain V., Dumont E., et. al.: Evaluation of liver diffusion isotropy and characterization of focal hepatic lesions with two single-shot echo-planar MR imaging sequences: prospective study in 66 patients. Radiology 2003; 226: pp. 71-78.