
Purpose
Targeted therapy can lead to considerable tumor reduction and may result initially in altered tissue at constant tumor size. In this setting, Response Evaluation Criteria in Solid Tumors (RECIST) can be inadequate for assessing early treatment response. Choi-criteria combine both size and density measurements. Our purpose was to evaluate computed tomography (CT) images of melanoma patients under BRAF-inhibitor therapy according to Choi-criteria which were adapted to our study (aChoi).
Material and Methods
Twelve patients (four male, eight female, mean age 49) with stage IV melanoma treated with a BRAF inhibitor were included. Response was assessed according to RECIST for 39 lesions in contrast-enhanced CT. Target volumes are semiautomatically segmented to calculate mean density for aChoi-criteria, thus using a two-dimensional nonstandardized region of interest could be prevented.
Results
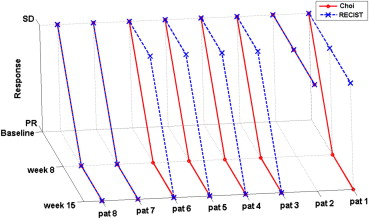
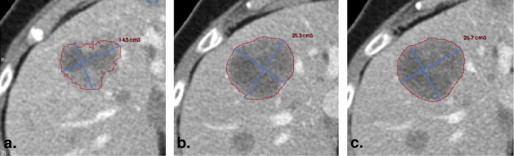
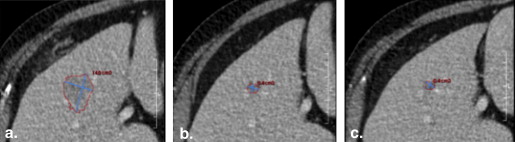
Eight patients are RECIST responders. aChoi-criteria indicate therapy response earlier compared to RECIST in five of eight patients. In seven cases, tumor density in CT had decreased 8 weeks after therapy start, whereas in some cases tumor size diminished less or even increased. Response according to aChoi was diagnosed in seven patients who showed in RECIST-evaluation stable disease in five and partial response in two cases. Fifteen weeks after therapy start almost all patients within the aChoi responders were RECIST responders, too. Only one aChoi responder showed still stable disease in RECIST.
Conclusion
Our initial data indicate that aChoi-criteria can reflect response to vemurafenib earlier compared to RECIST. This is of clinical significance as BRAF-inhibitors are cost-intensive targeted therapies and can cause severe side effects, so criteria for early therapy response have to be evaluated.
Incidence of melanoma is dramatically increasing , faster than any other cancer. The number of new diagnoses per year has doubling times up to 10–20 years . Unfortunately effects of chemotherapy in stage IV melanoma patients remain poor, showing less than a year median survival time . Looking for treatments improving prognosis of these patients, research focuses besides immunotherapies such as CTLA-4/PD-1 inhibitors on development of targeted therapies against mutated kinases such as BRAF and c-kit . An accurate assessment of tumor response to these targeted therapies is a major challenge, and it is unlikely that a single response evaluation criterion will be sufficient .
In 2011 a promising targeted therapy for patients with unresectable or metastatic melanoma has been approved by US Food and Drug Administration: vemurafenib (Zelboraf, Roche Pharma, Grenzach-Wyhlen) . The European Commission authorized this BRAF inhibitor in February 2012. BRAF is a cytoplasmic serine/threonine kinase in cellular signaling pathways . About 40%–60% of all melanoma patients show a V600E mutation in the BRAF kinase, in most cases leading to a substitution of glutamic acid by valine . Patients with this mutation can be successfully treated with vemurafenib, a small-molecule BRAF inhibitor . Oncogenic BRAF kinase is an important stimulator of metabolic activity , so inhibiting this enzyme results in modification of metabolism, as long as melanoma cells do not develop resistance . In a clinical phase I study of vemurafenib, the authors were able to relate this altered metabolism to decreased signal intensities in fluorodeoxyglucose–positron emission tomography (FDG-PET). In 81% of patients, significant reduction in FDG uptake was observed 2 weeks after therapy onset, before tumor regression could be measured .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Material and methods
Patient Population
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Response Evaluation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Imaging Technique
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Applied Amount of Contrast Media (Imeron 300, Bracco, Konstanz, Germany)
Body Weight (kg) Volume Contrast Media (mL) Flow Rate (mL/s) <55 85 3.1 55–64.9 115 3.5 65–90 130 4 >90 145 4.5
Get Radiology Tree app to read full this article<
Data Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 2
Size and Density Measurements of Target Lesions
Patient Baseline Follow-up 1 Follow-up 2 1n 4 SDT (mm) 133 137 147 Δ SDT (%) 3 11 SDET (HU) 76 62 59 Δ SDET (%) −18 −22 2n 4 SDT (mm) 80 75 70 Δ SDT (%) −6 −13 SDET (HU) 48 58 57 Δ SDET (%) 21 19 3n 2 SDT (mm) 39 28 16 Δ SDT (%) −28 −59 SDET (HU) 20 7 8 Δ SDET (%) −65 −60 4n 3 SDT (mm) 42 31 20 Δ SDT (%) −26 −52 SDET (HU) 82 53 28 Δ SDET (%) −35 −66 5n 5 SDT (mm) 125 95 82 Δ SDT (%) −24 −34 SDET (HU) 53 58 18 Δ SDET (%) 9 −66 6n 3 SDT (mm) 50 36 29 Δ SDT (%) −28 −42 SDET (HU) 41 39 32 Δ SDET (%) −5 −22 7n 3 SDT (mm) 77 38 31 Δ SDT (%) −51 −60 SDET (HU) 77 75 60 Δ SDET (%) −3 −22 8n 3 SDT (mm) 47 27 27 Δ SDT (%) −43 −43 SDET (HU) 93 84 104 Δ SDET (%) −10 12 9n SDT (mm) 135 96 144 Δ SDT (%) −29 7 SDET (HU) 64 39 48 Δ SDET (%) −39 −25 10n 3 SDT (mm) 91 110 Δ SDT (%) 21 SDET (HU) 76 82 Δ SDET (%) 8 11n 2 SDT (mm) 114 81 109 Δ SDT (%) −29 −4 SDET (HU) 79 48 70 Δ SDET (%) −39 −11 12n 2 SDT (mm) 41 48 61 Δ SDT (%) 17 49 SDET (HU) 108 57 56 Δ SDET (%) −47 −48
n, number of targets; SDT, sum of diameters of target lesions (mm); Δ SDT, change of SDT (%) compared to baseline; SDET, sum of densities of target lesions (HU); Δ SDET, change of SDET (%) compared to baseline.
Get Radiology Tree app to read full this article<
Nonprogressive Disease (Stable Disease, Partial Response, Complete Response)
Get Radiology Tree app to read full this article<
Table 3
Results
Patient Follow-up 1 Follow-up 2 1 RECIST SD SD Choi PR PR 2 RECIST SD SD Choi SD SD 3 RECIST SD PR Choi PR PR 4 RECIST SD PR Choi PR PR 5 RECIST SD PR Choi PR PR 6 RECIST SD PR Choi PR PR 7 RECIST PR PR Choi PR PR 8 RECIST PR PR Choi PR PR 9 RECIST SD PD Choi PR PD 10 RECIST PD Choi PD 11 RECIST SD PD Choi PR PD 12 RECIST SD PD Choi PR PD
SD, stable disease; PD, progressive disease; PR, partial response; RECIST, Response Evaluation Criteria in Solid Tumors.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Progressive Disease
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
References
1. Garbe C., Leiter U.: Melanoma epidemiology and trends. Clin Dermatol 2009; 27: pp. 3-9.
2. Lens M.B., Dawes M.: Global perspectives of contemporary epidemiological trends of cutaneous malignant melanoma. Br J Dermatol 2004; 150: pp. 179-185.
3. Balch C.M., Gershenwald J.E., Soong S.J., et. al.: Final version of 2009 AJCC melanoma staging and classification. J Clin Oncol 2009; 27: pp. 6199-6206.
4. Garbe C., Eigentler T.K., Keilholz U., et. al.: Systematic review of medical treatment in melanoma: current status and future prospects. Oncologist 2011; 16: pp. 5-24.
5. Figueiras R.G., Padhani A.R., Goh V.J., et. al.: Novel oncologic drugs: what they do and how they affect images. Radiographics 2011; 31: pp. 2059-2091.
6. Gray-Schopfer V., Wellbrock C., Marais R.: Melanoma biology and new targeted therapy. Nature 2007; 445: pp. 851-857.
7. Shanbhogue A.K., Karnad A.B., Prasad S.R.: Tumor response evaluation in oncology: current update. J Comp Assisted Tomogr 2010; 34: pp. 479-484.
8. Flaherty K.T., Yasothan U., Kirkpatrick P.: Vemurafenib. Nat Rev Drug Discov 2011; 10: pp. 811-812.
9. Bollag G., Hirth P., Tsai J., et. al.: Clinical efficacy of a RAF inhibitor needs broad target blockade in BRAF-mutant melanoma. Nature 2010; 467: pp. 596-599.
10. Davies H., Bignell G.R., Cox C., et. al.: Mutations of the BRAF gene in human cancer. Nature 2002; 417: pp. 949-954.
11. Flaherty K.T., Puzanov I., Kim K.B., et. al.: Inhibition of mutated, activated BRAF in metastatic melanoma. New Engl J Med 2010; 363: pp. 809-819.
12. Esteve-Puig R., Canals F., Colome N., et. al.: Uncoupling of the LKB1-AMPKalpha energy sensor pathway by growth factors and oncogenic BRAF. PloS one 2009; 4: pp. e4771.
13. Zheng B., Jeong J.H., Asara J.M., et. al.: Oncogenic B-RAF negatively regulates the tumor suppressor LKB1 to promote melanoma cell proliferation. Molec Cell 2009; 33: pp. 237-247.
14. Wan P.T., Garnett M.J., Roe S.M., et. al.: Mechanism of activation of the RAF-ERK signaling pathway by oncogenic mutations of B-RAF. Cell 2004; 116: pp. 855-867.
15. Nazarian R., Shi H., Wang Q., et. al.: Melanomas acquire resistance to B-RAF(V600E) inhibition by RTK or N-RAS upregulation. Nature 2010; 468: pp. 973-977.
16. Su F., Viros A., Milagre C., et. al.: RAS mutations in cutaneous squamous-cell carcinomas in patients treated with BRAF inhibitors. New Engl J Med 2012; 366: pp. 207-215.
17. Oberholzer P.A., Kee D., Dziunycz P., et. al.: RAS mutations are associated with the development of cutaneous squamous cell tumors in patients treated with RAF inhibitors. J Clin Oncol 2012; 30: pp. 316-321.
18. Choi H., Charnsangavej C., Faria S.C., et. al.: Correlation of computed tomography and positron emission tomography in patients with metastatic gastrointestinal stromal tumor treated at a single institution with imatinib mesylate: proposal of new computed tomography response criteria. J Clin Oncol 2007; 25: pp. 1753-1759.
19. Choi H.: Response evaluation of gastrointestinal stromal tumors. Oncologist 2008; 13: pp. 4-7.
20. Benjamin R.S., Choi H., Macapinlac H.A., et. al.: We should desist using RECIST, at least in GIST. J Clin Oncol 2007; 25: pp. 1760-1764.
21. Smith A.D., Shah S.N., Rini B.I., et. al.: Utilizing pre-therapy clinical schema and initial CT changes to predict progression-free survival in patients with metastatic renal cell carcinoma on VEGF-targeted therapy: a preliminary analysis. Urol Oncol 2011; Epub ahead of print
22. Eisenhauer E.A., Therasse P., Bogaerts J., et. al.: New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer 2009; 45: pp. 228-247.
23. Hurwitz H., Fehrenbacher L., Novotny W., et. al.: Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. New Engl J Med 2004; 350: pp. 2335-2342.
24. Llovet J.M., Di Bisceglie A.M., Bruix J., et. al.: Design and endpoints of clinical trials in hepatocellular carcinoma. J Natl Cancer Inst 2008; 100: pp. 698-711.
25. Wolchok J.D., Hoos A., O’Day S., et. al.: Guidelines for the evaluation of immune therapy activity in solid tumors: immune-related response criteria. Clin Cancer Res 2009; 15: pp. 7412-7420.
26. Chapman P.B., Hauschild A., Robert C., et. al.: Improved survival with vemurafenib in melanoma with BRAF V600E mutation. New Engl J Med 2011; 364: pp. 2507-2516.
27. Joseph E.W., Pratilas C.A., Poulikakos P.I., et. al.: The RAF inhibitor PLX4032 inhibits ERK signaling and tumor cell proliferation in a V600E BRAF-selective manner. Proc Natl Acad Sci USA 2010; 107: pp. 14903-14908.