
Rationale and Objectives
To evaluate the capability of cone-beam computed tomography (CBCT) acquired immediately after transcatheter arterial chemoembolization (TACE) in determining lipiodol retention quantitatively and volumetrically when compared to 1-day postprocedure unenhanced multidetector computed tomography (MDCT).
Materials and Methods
From June to December 2012, 15 patients met the inclusion criteria of unresectable hepatocellular carcinoma (HCC) that was treated with conventional TACE (cTACE) and had intraprocedural CBCT and 1-day post-TACE MDCT. Four patients were excluded because the lipiodol was diffuse throughout the entire liver or lipiodol deposition was not clear on both CBCT and MDCT. Eleven patients with a total of 31 target lesions were included in the analysis. A quantitative three-dimensional software was used to assess complete, localized, and diffuse lipiodol deposition. Tumor volume, lipiodol volume in the tumor, percent lipiodol retention, and lipiodol enhancement in Hounsfield units (HU) were calculated and compared between CBCT and MDCT using two-tailed Student’s t test and Bland–Altman plots.
Results
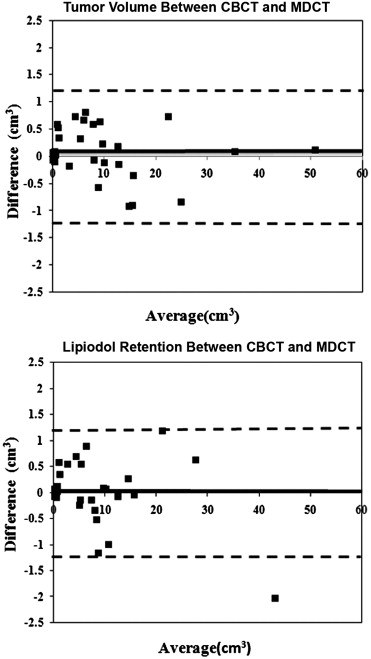
The mean value of tumor volume, lipiodol-deposited regions, calculated average percent lipiodol retention, and HU value of CBCT were not significantly different from those of MDCT (tumor volume: 9.37 ± 11.35 cm 3 vs 9.34 ± 11.44 cm 3 , P = .991; lipiodol volume: 7.84 ± 9.34 cm 3 vs 7.84 ± 9.60 cm 3 , P = .998; lipiodol retention: 89.3% ± 14.7% vs. 90.2% ± 14.9%, P = .811; HU value: 307.7 ± 160.1 HU vs. 257.2 ± 120.0 HU, P = .139). Bland–Altman plots showed only minimal difference and high agreement when comparing CBCT to MDCT.
Conclusions
CBCT has a similar capability, intraprocedurally, to assess lipiodol deposition in three dimensions for patients with HCC treated with cTACE when compared to MDCT.
Hepatocellular carcinoma (HCC) is the sixth most prevalent cancer worldwide and the third most common cancer leading to death. However, only a minority of all patients with HCC are surgical candidates at the time of diagnosis . Transcatheter arterial chemoembolization (TACE) is one of the most commonly used intra-arterial therapies to treat unresectable HCC, and several clinical trials have demonstrated that TACE has the potential to show survival benefits in patients with HCC . Conventional TACE (cTACE) is a frequently used technique and usually includes intra-arterial delivery of emulsions mixed with chemotherapeutic agents and lipiodol, followed by the administration of the embolic agent. It has been demonstrated that the degree of intratumoral lipiodol deposition correlates well with tumor necrosis, tumor recurrence, and survival rate after TACE . Fluoroscopic imaging is widely used to assess the lipiodol accumulation during and immediately after TACE. However, this modality has several limitations for the assessment of lipiodol retention because it cannot provide volumetric information, as does cross-sectional imaging. An alternative method for the evaluation of lipiodol accumulation is unenhanced multidetector computed tomography (MDCT) imaging. MDCT can be more accurate to assess lipiodol accumulation in HCC when compared to fluoroscopy imaging and is routinely used to evaluate the lipiodol deposition within 1 week after TACE.
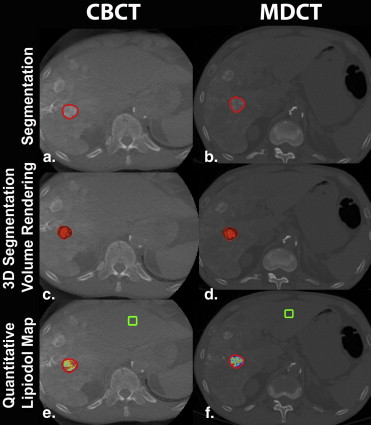
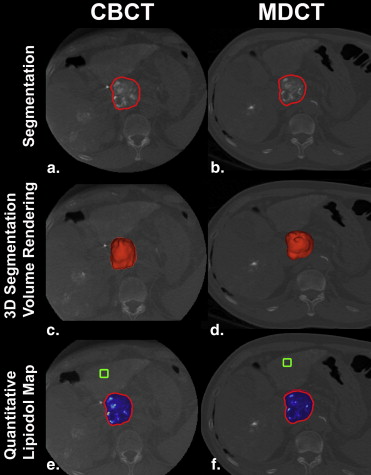
The advent and development of cone-beam computed tomography (CBCT) technology provide interventional radiologists with an intraprocedural method to volumetrically assess lipiodol retention. CBCT offers soft tissue cross-sectional imaging using a flat-panel detector. It provides volumetric information about tumor location, number, and vascularity and can be used for real-time image guidance as well as to predict tumor response . Compared to MDCT, CBCT has several unique advantages, such as a lower dose of x-ray exposure and convenience for immediately assessing lipiodol accumulation after TACE . Iwazawa et al recently showed CBCT is nearly equivalent to MDCT to detect incomplete lipiodol accumulation using a semiquantitative visual grading score. However, several drawbacks existed in this study. For example, the parameters were semiquantitative, and diffuse lipiodol retention in the tumor was not taken into account. In addition, MDCT was performed 1 week after the procedure. Furthermore, recent work has been done by Chen et al to better quantify the lipiodol retention, but the study was bidimensional (2D) . To address these limitations, we build on both works using a quantitative and volumetric three-dimensional (3D) semiautomatic software. This software can more clearly visualize the degree of lipiodol deposition within the targeted lesion using color-coding and can automatically calculate three-dimensionally, both the volume of the tumor and the volume of the lipiodol deposition, even for diffuse retention in CBCT and MDCT. The purpose of this study is to quantify the capability of CBCT acquired immediately after cTACE to assess lipiodol retention in three dimensions for patients with HCC when compared to unenhanced MDCT.
Materials and methods
Patient Selection
Get Radiology Tree app to read full this article<
Transcatheter Arterial Chemoembolization
Get Radiology Tree app to read full this article<
CBCT Imaging
Get Radiology Tree app to read full this article<
MDCT Imaging
Get Radiology Tree app to read full this article<
Semiautomatic Segmentation of Tumor and Lipiodol Retention
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Automatic Measurement of Complete, Localized, and Diffuse Lipiodol Retention
Get Radiology Tree app to read full this article<
Statistics
Get Radiology Tree app to read full this article<
Results
Patient Demographics
Get Radiology Tree app to read full this article<
Lipiodol Conspicuity in the Tumor
Get Radiology Tree app to read full this article<
Tumor and Lipiodol Volume on CBCT and MDCT
Get Radiology Tree app to read full this article<
Table 1
Tumor and Lipiodol Volume and Percentage of Lipiodol to Tumor as Measured on Cone-beam Computed Tomography (CBCT) and Multidetector Computed Tomography (MDCT)
CBCT MDCT_P_ Value Tumor volume (cm 3 ) 9.37 ± 11.35 9.34 ± 11.44 .991 Lipiodol volume (cm 3 ) 7.84 ± 9.34 7.84 ± 9.60 .998 Percentage of lipiodol retention 89.3% ± 14.7% 90.2% ± 14.9% .811
Data were expressed as mean ± SD.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Forner A., Llovet J.M., Bruix J.: Hepatocellular carcinoma. Lancet 2012; 379: pp. 1245-1255.
2. Marín-Hargreaves G., Azoulay D., Bismuth H.: Hepatocellular carcinoma: surgical indications and results. Crit Rev Oncol Hematol 2003; 47: pp. 13-27.
3. Lo C.M., Ngan H., Tso W.K., et. al.: Randomized controlled trial of transarterial lipiodol chemoembolization for unresectable hepatocellular carcinoma. Hepatology 2002; 35: pp. 1164-1171.
4. Brown D.B., Geschwind J.F., Soulen M.C., et. al.: Society of Interventional Radiology position statement on chemoembolization of hepatic malignancies. J Vasc Interv Radiol 2006; 17: pp. 217-223.
5. Monsky W.L., Kim I., Loh S., et. al.: Semiautomated segmentation for volumetric analysis of intratumoral ethiodol uptake and subsequent tumor necrosis after chemoembolization. AJR Am J Roentgenol 2010; 195: pp. 1220-1230.
6. Takayasu K., Muramatsu Y., Maeda T., et. al.: Targeted transarterial oily chemoembolization for small foci of hepatocellular carcinoma using a unified helical CT and angiography system: analysis of factors affecting local recurrence and survival rates. AJR Am J Roentgenol 2001; 176: pp. 681-688.
7. Lee H.S., Kim K.M., Yoon J.H., et. al.: Therapeutic efficacy of transcatheter arterial chemoembolization as compared with hepatic resection in hepatocellular carcinoma patients with compensated liver function in a hepatitis B virus endemic area: a prospective cohort study. J Clin Oncol 2002; 20: pp. 4459-4465.
8. Tognolini A., Louie J.D., Hwang G.L., et. al.: Utility of C-arm CT in patients with hepatocellular carcinoma undergoing transhepatic arterial chemoembolization. J Vasc Interv Radiol 2010; 21: pp. 339-347.
9. Higashihara H., Osuga K., Onishi H., et. al.: Diagnostic accuracy of C-arm CT during selective transcatheter angiography for hepatocellular carcinoma: comparison with intravenous contrast-enhanced, biphasic, dynamic MDCT. Eur Radiol 2012; 22: pp. 872-879.
10. Loffroy R., Lin M., Yenokyan G., et. al.: Intraprocedural C-arm dual-phase cone-beam CT: can it be used to predict short-term response to TACE with drug-eluting beads in patients with hepatocellular carcinoma?. Radiology 2013; 266: pp. 636-648.
11. Kim S., Yoshizumi T.T., Toncheva G., et. al.: Comparison of radiation doses between cone beam CT and multi detector CT: TLD measurements. Radiat Prot Dosimetry 2008; 132: pp. 339-345.
12. Iwazawa J., Ohue S., Kitayama T., et. al.: C-arm CT for assessing initial failure of iodized oil accumulation in chemoembolization of hepatocellular carcinoma. AJR Am J Roentgenol 2011; 197: pp. W337-W342.
13. Chen R., Geschwind J.F., Wang Z., et. al.: Quantitative assessment of lipiodol deposition after chemoembolization between cone-beam CT and multidetector CT. J Vasc Interv Radiol 2013; 24: pp. 1837-1844.
14. Sultana S., Awai K., Nakayama Y., et. al.: Hypervascular hepatocellular carcinomas: bolus tracking with a 40-detector CT scanner to time arterial phase imaging. Radiology 2007; 243: pp. 140-147.
15. Tacher V., Lin M., Chao M., et. al.: Semiautomatic volumetric tumor segmentation for hepatocellular carcinoma: comparison between C-arm cone beam computed tomography and MRI. Acad Radiol 2013; 20: pp. 446-452.
16. Pellerin O., Lin M., Bhagat N., et. al.: Comparison of semi-automatic volumetric VX2 hepatic tumor segmentation from cone beam CT and multi-detector CT with histology in rabbit models. Acad Radiol 2013; 20: pp. 115-121.
17. Taguchi K., Funama Y., Zhang M., et. al.: Quantitative measurement of iodine concentration in the liver using abdominal C-arm computed tomography. Acad Radiol 2009; 16: pp. 200-208.
18. Lin M., Pellerin O., Bhagat N., et. al.: Quantitative and volumetric EASL and RECIST: feasibility of a semi-automated software method to assess tumor response after transcatheter arterial chemoembolization (TACE). J Vasc Interv Radiol 2012; 23: pp. 1629-1637.
19. Takayasu K., Arii S., Matsuo N., et. al.: Comparison of CT findings with resected specimens after chemoembolization with iodized oil for hepatocellular carcinoma. AJR Am J Roentgenol 2000; 175: pp. 699-704.
20. El Khaddari S., Gaudin J.L., Abidi H., et. al.: Chemoembolization in hepatocellular carcinoma: multivariate analysis of survival prognostic factors after the first session. Gastroenterol Clin Biol 2002; 26: pp. 728-734.
21. Kim D.Y., Ryu H.J., Choi J.Y., et. al.: Radiological response predicts survival following transarterial chemoembolization in patients with unresectable hepatocellular carcinoma. Aliment Pharmacol Ther 2012; 35: pp. 1343-1350.
22. Meyer B.C., Frericks B.B., Voges M., et. al.: Visualization of hypervascular liver lesions during TACE: comparison of angiographic C-arm CT and MDCT. AJR Am J Roentgenol 2008; 190: pp. W263-W269.
23. Iwazawa J., Ohue S., Hashimoto N., et. al.: Survival after C-arm CT-assisted chemoembolization of unresectable hepatocellular carcinoma. Eur J Radiol 2012; 81: pp. 3985-3992.
24. Miyayama S., Yamashiro M., Hashimoto M., et. al.: Comparison of local control in transcatheter arterial chemoembolization of hepatocellular carcinoma ≤6 cm with or without intraprocedural monitoring of the embolization area using cone-beam computed tomography. Cardiovasc Intervent Radiol 2013 Jun 19; [Epub ahead of print]
25. Sun J.H., Wang L.G., Bao H.W., et. al.: Usefulness of C-arm angiographic computed tomography for detecting iodized oil retention during transcatheter arterial chemoembolization of hepatocellular carcinoma. J Int Med Res 2010; 38: pp. 1259-1265.
26. Loffroy R., Lin M., Rao P., et. al.: Comparing the detectability of hepatocellular carcinoma by C-arm dual-phase cone-beam computed tomography during hepatic arteriography with conventional contrast-enhanced magnetic resonance imaging. Cardiovasc Intervent Radiol 2012; 35: pp. 97-104.
27. Akpek S., Brunner T., Benndorf G., et. al.: Three-dimensional imaging and cone beam volume CT in C-arm angiography with flat panel detector. Diagn Interv Radiol 2005; 11: pp. 10-13.