
Rationale and Objectives
To investigate the response after magnetic resonance–guided high-intensity focused ultrasound (MRgHIFU) treatment of uterine fibroids (UF) using a three-dimensional (3D) quantification of total and enhancing lesion volume (TLV and ELV, respectively) on contrast-enhanced MRI (ceMRI) scans.
Methods and Materials
In a total of 24 patients, ceMRI scans were obtained at baseline and 24 hours, and 6, 12, and 24 months after MRgHIFU treatment. The dominant lesion was assessed using a semiautomatic quantitative 3D segmentation technique. Agreement between software-assisted and manual measurements was then analyzed using a linear regression model. Patients were classified as responders (R) or nonresponders (NR) on the basis of their symptom report after 6 months. Statistical analysis included the paired t –test and Mann–Whitney test.
Results
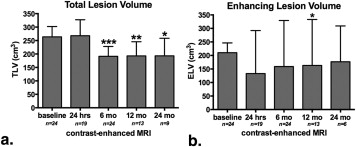
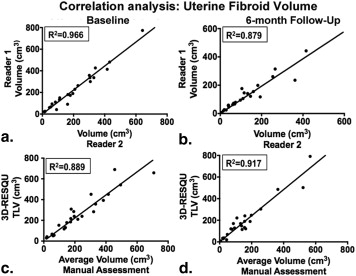
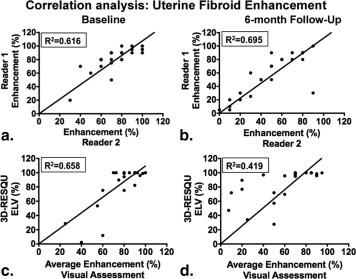
Preprocedurally, the median TLV and ELV were 263.74 cm 3 (30.45–689.56 cm 3 ) and 210.13 cm 3 (14.43–689.53 cm 3 ), respectively. The 6-month follow-up demonstrated a reduction of TLV in 21 patients (87.5%) with a median TLV of 171.7 cm 3 (8.5–791.2 cm 3 ; P < .0001). TLV remained stable with significant differences compared to baseline ( P < .001 and P = .047 after 12 and 24 months). A reduction of ELV was apparent in 16 patients (66.6%) with a median ELV of 158.91 cm 3 (8.55–779.61 cm 3 ) after 6 months ( P = .065). Three-dimensional quantification and manual measurements showed strong intermethod agreement for fibroid volumes ( R 2 = .889 and .917) but greater discrepancy for enhancement calculations ( R 2 = .659 and .419) at baseline and 6 months. No significant differences in TLV or ELV were observed between clinical R ( n = 15) and NR ( n = 3).
Conclusions
The 3D assessment has proven feasible and accurate in the quantification of fibroid response to MRgHIFU. Contrary to ELV, changes in TLV may be representative of the clinical outcome.
Uterine fibroids (UF) represent one of the most common benign tumors that predominantly occur in the perimenopausal years . Location, size, and multiplicity of UF are varying, resulting in a diversity of clinical presentations that range from asymptomatic to symptoms which highly interfere with the patient’s quality of life . As for the treatment of UF, surgical removal (myomectomy or hysterectomy) remains the gold standard, and UF represents the major indication for hysterectomy . However, there are minimal invasive treatment options including radiofrequency ablation and catheter-based approaches, such as uterine artery (UAE), which have become well-accepted alternatives to surgery over the last decades .
Magnetic resonance–guided high-intensity focused ultrasound (MRgHIFU) represents another approach and is the only fully noninvasive alternative in the treatment of UF. MRgHIFU uses targeted energy deposition from focused ultrasound under MR guidance to ablate the tissue by thermal coagulation and acoustic cavitation . MRgHIFU has proved as safe, feasible, and effective in reducing clinical symptoms .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Study Cohort
Get Radiology Tree app to read full this article<
Clinical Evaluation
Get Radiology Tree app to read full this article<
MRgHIFU Procedure and Follow-up Imaging
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
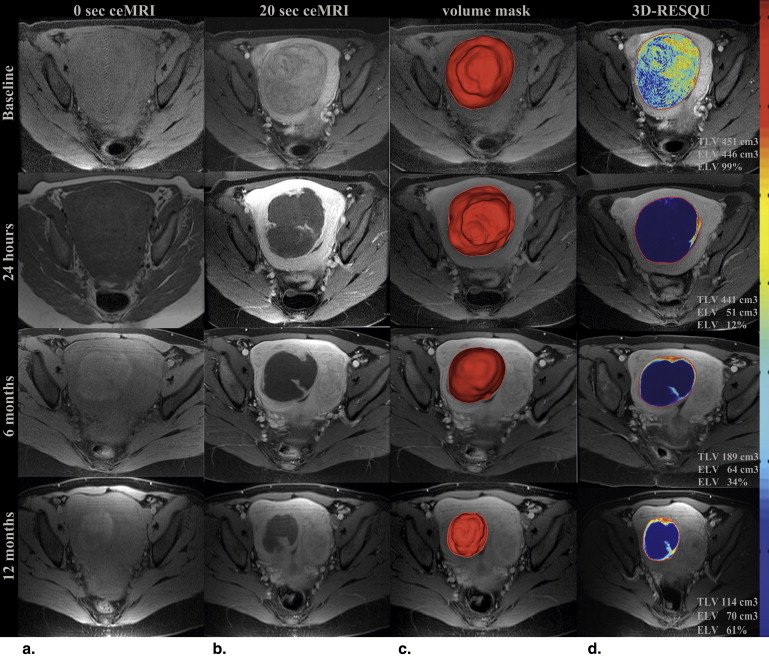
Imaging Data Evaluation—3D Quantification of Lesion Response
Lesion Segmentation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
3D-RESQU Technique
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Manual Image Analysis
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Study Population
Get Radiology Tree app to read full this article<
Table 1
Patient Characteristics
Parameter Study Population, n Age ( n = 24) 46.13 ∗ years (range, 37–53) Race African American 9 White 13 Other 2 Clinical symptoms at presentation (n = 19) Menorrhagia 13 (68%) Bulk-related symptoms 16 (84%) Number of uterine fibroids 1 9 2 9 >2 6 Baseline TLV ( n = 24) 263.74 ∗ cm 3 (range, 30.45–689.56)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Imaging Results
Volumetric Assessment I—TLV
Get Radiology Tree app to read full this article<
Volumetric Assessment II—ELV
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Manual and Visual Image Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Clinical Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Cramer S.F., Patel A.: The frequency of uterine leiomyomas. Am J Clin Pathol 1990; 94: pp. 435-438. PubMed PMID: 2220671
2. Flake G.P., Andersen J., Dixon D.: Etiology and pathogenesis of uterine leiomyomas: a review. Environ Health Perspect 2003; 111: pp. 1037-1054. PubMed PMID: 12826476; PubMed Central PMCID: PMCPMC1241553
3. Kröncke T., David M.: [Uterine artery embolization (UAE) for fibroid treatment: results of the 4th Radiological Gynecological Expert Meeting]. Rofo 2013; 185: pp. 461-463. PubMed PMID: 23572203
4. Kröncke T.J., Hamm B.: [Role of magnetic resonance imaging (MRI) in establishing the indication for, planning, and following up uterine artery embolization (UAE) for treating symptomatic leiomyomas of the uterus]. Radiologe 2003; 43: pp. 624-633. PubMed PMID: 14504762
5. ter Haar G.: High intensity ultrasound. Semin Laparosc Surg 2001; 8: pp. 77-89. PubMed PMID: 11337740
6. ter Haar G.: Ultrasound bioeffects and safety. Proc Inst Mech Eng H 2010; 224: pp. 363-373. PubMed PMID: 20349824
7. Fan R., Zhu L., Gong X.M., et. al.: [Prospective study on magnetic resonance-guided focused ultrasound surgery for symptomatic uterine fibroid: short-term follow up]. Zhonghua Fu Chan Ke Za Zhi 2013; 48: pp. 183-187. PubMed PMID: 23849940
8. Stewart E.A., Rabinovici J., Tempany C.M., et. al.: Clinical outcomes of focused ultrasound surgery for the treatment of uterine fibroids. Fertil Steril 2006; 85: pp. 22-29. PubMed PMID: 16412721
9. Kim H.S., Baik J.H., Pham L.D., et. al.: MR-guided high-intensity focused ultrasound treatment for symptomatic uterine leiomyomata: long-term outcomes. Acad Radiol 2011; 18: pp. 970-976. PubMed PMID: 21718955; PubMed Central PMCID: PMCPMC3401073
10. Kroencke T.J., Scheurig C., Poellinger A., et. al.: Uterine artery embolization for leiomyomas: percentage of infarction predicts clinical outcome. Radiology 2010; 255: pp. 834-841. PubMed PMID: 20392986
11. Fennessy F.M., Tempany C.M., McDannold N.J., et. al.: Uterine leiomyomas: MR imaging-guided focused ultrasound surgery—results of different treatment protocols. Radiology 2007; 243: pp. 885-893. PubMed PMID: 17446521
12. Spies J.B., Coyne K., Guaou Guaou N., et. al.: The UFS-QOL, a new disease-specific symptom and health-related quality of life questionnaire for leiomyomata. Obstet Gynecol 2002; 99: pp. 290-300. PubMed PMID: 11814511
13. Tacher V., Lin M., Chao M., et. al.: Semiautomatic volumetric tumor segmentation for hepatocellular carcinoma: comparison between C-arm cone beam computed tomography and MRI. Acad Radiol 2013; 20: pp. 446-452. PubMed PMID: 23498985; PubMed Central PMCID: PMCPMC3602801
14. Duran R., Chapiro J., Frangakis C., et. al.: Uveal melanoma metastatic to the liver: the role of quantitative volumetric contrast-enhanced MR imaging in the assessment of early tumor response after transarterial chemoembolization. Transl Oncol 2014; PubMed PMID: 24953419
15. Chapiro J., Wood L.D., Lin M., et. al.: Radiologic-pathologic analysis of contrast-enhanced and diffusion-weighted MR imaging in patients with HCC after TACE: diagnostic accuracy of 3D quantitative image analysis. Radiology 2014; pp. 140033. PubMed PMID: 25028783
16. Froeling V., Meckelburg K., Schreiter N.F., et. al.: Outcome of uterine artery embolization versus MR-guided high-intensity focused ultrasound treatment for uterine fibroids: long-term results. Eur J Radiol 2013; 82: pp. 2265-2269. PubMed PMID: 24075785
17. Yoon S.W., Cha S.H., Ji Y.G., et. al.: Magnetic resonance imaging-guided focused ultrasound surgery for symptomatic uterine fibroids: estimation of treatment efficacy using thermal dose calculations. Eur J Obstet Gynecol Reprod Biol 2013; 169: pp. 304-308. PubMed PMID: 23523412
18. Hesley G.K., Gorny K.R., Woodrum D.A.: MR-guided focused ultrasound for the treatment of uterine fibroids. Cardiovasc Intervent Radiol 2013; 36: pp. 5-13. PubMed PMID: 22453202
19. Goodwin S.C., Vedantham S., McLucas B., et. al.: Preliminary experience with uterine artery embolization for uterine fibroids. J Vasc Interv Radiol 1997; 8: pp. 517-526. PubMed PMID: 9232565
20. Greenwood L.H., Glickman M.G., Schwartz P.E., et. al.: Obstetric and nonmalignant gynecologic bleeding: treatment with angiographic embolization. Radiology 1987; 164: pp. 155-159. PubMed PMID: 3495816
21. Keshavarzi A., Vaezy S., Noble M.L., et. al.: Treatment of uterine fibroid tumors in an in situ rat model using high-intensity focused ultrasound. Fertil Steril 2003; 80: pp. 761-767. PubMed PMID: 14505751
22. Kaufman C., Pollak J., Mojibian H.: What is too big? Uterine artery embolization of a large fibroid causing abdominal compartment syndrome. Semin Intervent Radiol 2014; 31: pp. 207-211. PubMed PMID: 25049449; PubMed Central PMCID: PMCPMC4078127
23. Spies J.B., Roth A.R., Jha R.C., et. al.: Leiomyomata treated with uterine artery embolization: factors associated with successful symptom and imaging outcome. Radiology 2002; 222: pp. 45-52. PubMed PMID: 11756703