
Highlights
Standardizing diagnostic test-related benefits and risks may improve decision making.
Benefit-risk assessment (BRA) in diagnostic radiology involves multiple criteria.
We propose a framework and process based on using standardized benefit-risk criteria (BRC).
Multi-disciplinary teams of radiologists and imaging-ordering providers may improve decisions.
Rationale and Objectives
Get Radiology Tree app to read full this article<
Materials and Methods
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Introduction
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Methods
Get Radiology Tree app to read full this article<
Literature Search
Get Radiology Tree app to read full this article<
Creation and Design of Survey
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Selection of Clinical Scenarios
Get Radiology Tree app to read full this article<
Survey Respondent Identification and Recruitment
Get Radiology Tree app to read full this article<
Selection of BRC for Clinical Scenarios
Get Radiology Tree app to read full this article<
A patient seeks diagnosis for non-specific, subacute low back pain. The patient has had non-specific pain for more than 3 months but has no history of structural problems or trauma, leg pain or red flags. You are asked to weigh the benefits and harms of two diagnostic approaches: Approach A: magnetic resonance imaging (MRI) Approach B: no additional diagnostic or therapeutic action (No Test) For each reason listed below select MRI if MRI offers an advantage over No Test, select No Test if No Test offers an advantage over MRI and select N/A if comparison is not possible or there is no meaningful difference between approaches.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Literature Search
Get Radiology Tree app to read full this article<
Online Survey Responses
Get Radiology Tree app to read full this article<
TABLE 1
Description of Clinical Conditions Presented in the Survey
ACR AC Clinical Scenarios Survey Description of Case Comparators Clinical Specialties Recruited Low back pain (NGC-8863) variant 1 A patient seeks diagnosis for nonspecific, subacute lower back pain. The patient has had nonspecific pain for more than 3 months but has no history of structural problems or trauma, leg pain, or red flags. Magnetic resonance imaging (MRI) compared to no testing Neuroradiology and primary care Chronic headache, no new features (NGC-7779) variant 1 A patient seeks diagnosis for chronic uncomplicated headache. The patient is not experiencing new headache features, focal neurologic deficits, or red flags. Magnetic resonance imaging (MRI) compared to no testing Neuroradiology and primary care Lower quadrant pain-suspected appendicitis (NGC-10146) variant 1 A patient arrives complaining of lower quadrant pain. Fever, leukocytosis, and other signs point to a classic case of clinical appendicitis. Ultrasound (US) compared to computed tomography (CT) Emergency medicine and emergency radiology Acute-onset flank pain suspicion of stone disease (NGC-008476) variant 2 A patient arrives complaining of acute-onset flank pain. The patient is having recurrent symptoms of stone disease. Ultrasound (US) compared to computed tomography (CT) Emergency medicine and emergency radiology
AC, Appropriateness Criteria; ACR, American College of Radiology; NGC, National Guideline Clearinghouse.
Get Radiology Tree app to read full this article<
The Finalized BRC Domains and Criteria
Get Radiology Tree app to read full this article<
TABLE 2
Test-specific Features Domain BRC
Criteria Brief Description Missed cases Type II error or as 1-NPV (the chance of having the condition among those who test negative) False diagnoses Type I error or 1-PPV (the chance of not having the condition among those who test positive) Diagnostic accuracy consistency Existence/extent of influence of patient characteristics on diagnostic accuracy Interobserver reading agreement Proxy measure of image clarity and quality Depth/breadth of anatomy visualization Categorization of extent of anomaly characterization (eg, size, shape, vascularization, shape) Invasiveness/risk of adverse events The number or categorization of probabilities and/or severity of adverse events Contrast reaction potential Probability or categorization of probability and/or severity of contrast reaction Ionizing radiation dose Measure of millisievert dose or categorization of dose Patient-specific exclusions Measure of existence/extent categorization of exclusions (eg, metal implants, BMI, age) Failure/malfunction rate Failure rate or categorization of the rate/manufacturer reputation Patient preparation requirements Number of minutes or categorization of relative wait times Examination time Number of minutes or categorization of relative wait times Posttest observation time Number of minutes or categorization of relative wait times Decision support Existence/extent of automated interpretation or characterization of function Portability Existence/extent of device portability Ease of use Categorization of dependence on skilled operator Reimbursement potential Categorization of relative potential for reimbursement
BMI, body mass index; BRC, benefit-risk criteria; NPV, negative predictive value; PPV, positive predictive value.
Get Radiology Tree app to read full this article<
Test-specific Features ( N = 17)
Get Radiology Tree app to read full this article<
Patient Management and Provider Intrinsic Value ( N = 12)
Get Radiology Tree app to read full this article<
TABLE 3
Patient Management and Provider Intrinsic Value BRC
Criteria Brief Description Therapeutic/procedural success Net counts/probability and severity/categorization of complications of medical treatment with/without test Potential for additional confirmatory testing (inconclusive/false-positive results) Existence/extent of confirmatory testing Potential for incidental finding management Existence/extent of repeat follow-up Net unnecessary treatment (test prescribed or averted treatment) Net counts/probability and severity/categorization of unnecessary treatments performed or averted based on test information Access to test Perceived relative access to test Time to diagnosis Net hours/days/weeks to diagnosis or extent of delay with/without test Inpatient/outpatient healthcare visits Net number of healthcare visits or extent of utilization with/without test Time to discharge Net hours/days/weeks to discharge with/without test Provider utility Extent of confidence in test usefulness Liability protections Existence/extent of protection from liability afforded by test Financial incentives Existence/extent associated with test Contribution of information to prognosis Existence/extent of test information contributing to prognosis
BRC, benefit-risk criteria.
Get Radiology Tree app to read full this article<
Patient Intrinsic Value and Outcomes ( N = 7)
Get Radiology Tree app to read full this article<
TABLE 4
Patient Outcomes and Intrinsic Value Domain BRC
Criteria Brief Description Value of knowing Value of knowing true test results; decrease in perceived uncertainty (eg, peace of mind, reassurance) Disvalue of knowing Disvalue of knowing false test results or learning of insignificant incidental findings; increase in perceived uncertainty (eg, anxiety, confusion, distrust) Burden (time and money) to patient Out-of-pocket travel costs and work absenteeism: direct time and money costs of test Patient comfort Claustrophobia, fasting, physical discomfort, and pain from test Patient future compliance and behavior Changes in behavior: measures of uptake or attrition of health visits/programs Radiation-induced cancers Count of expected cases/QALYs lost Length/quality of life Net incremental survival attributable to test/net QALYs
BRC, benefit-risk criteria; QALYs, quality-adjusted life-years.
Get Radiology Tree app to read full this article<
Additional Considerations
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Clinical Scenarios
Get Radiology Tree app to read full this article<
TABLE 5
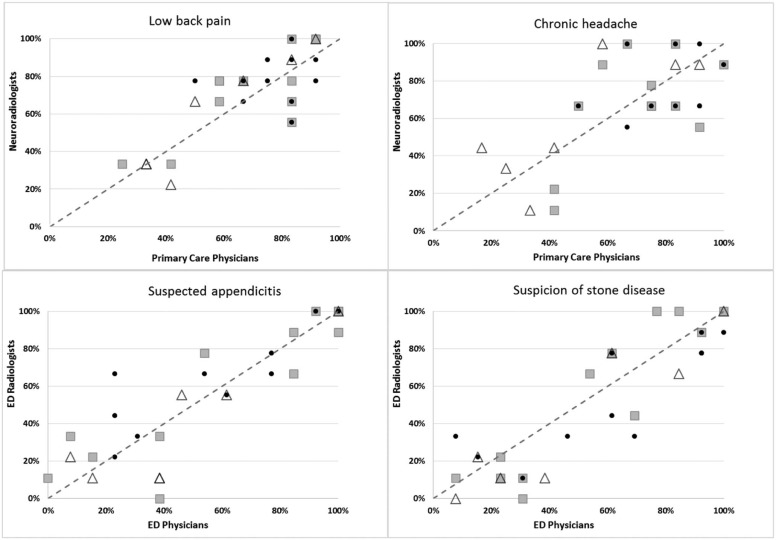
Survey Results by Clinical Scenario and Specialty
Domain Initial List of Benefit-risk Criteria Low Back Pain Chronic Headache Suspected Appendicitis Suspicion of Stone Disease PCP NRAD PCP NRAD ED MD ED RAD ED MD ED RAD TSF Manufacturer reputation ◐ ◐ ◐ ○ ○ ○ ○ ○Missed cases ● ● ● ● ● ● ● ● False diagnoses ● ● ● ● ◕ ● ◕ ◕ Patient preparation requirements ● ● ● ◕ ◐ ◐ ◐ ○ Diagnostic accuracy consistency ◕ ● ◕ ● ● ● ● ● Invasiveness/risk of adverse events ● ◕ ● ◕ ● ◕ ◕ ◐ Contrast reaction potential ● ◕ ● ◕ ● ● ◕ ● Ionizing radiation dose ○ ◐ ◐ ○ ● ● ● ● Failure/malfunction rate ◕ ● ● ● ○ ◐ ○ ○ Decision support features ◕ ● ● ◕ ◐ ○ ◐ ○ Portability of the device ◕ ◕ ◐ ◕ ● ● ● ● Reimbursement potential ● ● ◕ ● ○ ○ ○ ○ PMPV Therapeutic/procedural success ● ● ◐ ◕ ○ ◕ ◐ ◐Potential for additional confirmatory testing ● ● ● ● ● ● ● ●Provider utility ● ● ● ● ● ● ● ● Potential for incidental findings management ● ● ● ◕ ● ● ● ● Net unnecessary treatment ● ● ● ◕ ◕ ◕ ◕ ◐ Time to diagnosis ● ● ● ◕ ◕ ◕ ◕ ● Inpatient/outpatient healthcare visits ● ◕ ● ◕ ○ ◐ ◐ ○ Time to discharge ◕ ◕ ◐ ◕ ◐ ◐ ○ ○ Liability protections ● ◕ ● ● ● ◕ ◕ ◐ Financial incentives ◐ ● ◕ ◕ ○ ○ ○ ◐ Contribution of information to prognosis ◕ ● ◕ ● ● ● ● ● POIV Value of knowing ◕ ● ◕ ● ◐ ◕ ● ◕ Disvalue of knowing ● ● ● ● ◐ ○ ◐ ○ Burden (time and money) to patient ● ● ● ● ◕ ◕ ◕ ● Patient future compliance and behavior ◐ ○ ○ ◐ ○ ○ ○ ○ Radiation-induced cancers ◐ ◐ ◐ ○ ● ● ● ● Quality of life ◐ ◕ ◐ ◐ ○ ○ ○ ○ Length of life ◐ ◐ ○ ◐ ◐ ○ ○ ○ Consensus percentages indicating respondents believed there were differences between testing strategies (MRI vs no testing or CT vs US), stratified by clinical scenario and specialty <25% 25%–50% 51%–75% >75% ○ ◐ ◕ ●
CT, computed tomography; ED MD, emergency department medical doctor; ED RAD, emergency radiologist; MRI, magnetic resonance imaging; NRAD, neuroradiologist; PCP, primary care provider; PMPV, patient management and provider intrinsic value; POIV, patient outcomes and intrinsic value; TSF, test-specific features; US, ultrasound.
Patient comfort, interobserver reading agreement, depth/breadth of anatomy visualization, patient-specific exclusions, patient preparation requirements, examination time, posttest observation time, ease of use, access to test, and time to diagnosis were added to the final list based on short answer responses on the survey. Manufacturer reputation removed from the final list.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
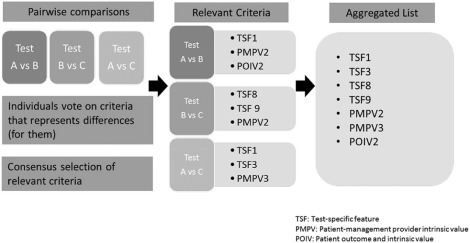
The Proposed Framework: Consensus-based Selection of Relevant BRC
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Step 1: Pairwise Comparisons Based on Individual Beliefs
Get Radiology Tree app to read full this article<
Step 2: Consensus Selection of Relevant Criteria
Get Radiology Tree app to read full this article<
Step 3: Group Review of the Aggregated List
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
Appendix
Get Radiology Tree app to read full this article<
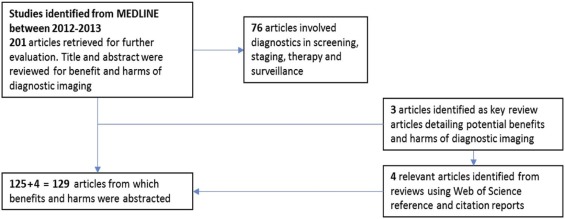
TABLE A1
Literature Search Results Mapped to the Fryback and Thornbury Hierarchical Model of Efficacy
Technical efficacy
The design and technical performance of test
Resolution of line pairs
Modulation of transfer function change
Gray scale range
Amount of mottle
Sharpness
Reliability of image quality and performance
Performance dependencies (multiple tests relying on one another for effectiveness)
Patient wait/preparation time for test
Length of examination
Post-test observation time
Inconclusive results Diagnostic accuracy efficacy
Yield of abnormal or normal diagnoses in case series
Diagnostic accuracy
Positive and negative predictive value
Sensitivity and specificity in a clinical case
ROC Positive and negative predictive values (47 references)
Positive likelihood ratio
Diagnostic odds ratio
Detection percentage
Accuracy in subpopulations Diagnostic thinking efficacy
Impact on pretest probability
Probability of learning incidental information Provider confidence
Liability avoidance
Risk stratification
Probability of learning incidental information
Pre-test probability Therapeutic efficacy
How helpful an imaging test is to patient management
Unnecessary procedures avoided
Pre-test/post-test therapy changes Procedural success
Number of healthcare visits
Need for additional follow-up
Downstream procedures from incidental findings
Radiation exposure dose
Extent and severity of harms associated with unnecessary procedures Patient outcome efficacy
Morbidity (procedures) avoided in QALYs
Patient improvement with vs. without test
Survival measured in QALYs
Value of test information to patient (future planning and psychological impact)
Cost per QALY saved with image information Pain and other physical discomfort such as tight quarters
Psychological impact (e.g. anxiety, reassurance or peace of mind)
Future planning based on test information
Tolerability
Sequelae from contrast reagent reactions
Invasiveness
Patient compliance (downstream)
Morbidity and mortality benefit from improved treatment plan
Radiation-associated cancers
Non-institutionalized days alive
Quality of life
ROC, receiver operating characteristic; QALYs, quality-adjusted life-years.
Societal efficacy, the last tier of the hierarchy, is not represented, as costs are not typically considered in benefit-risk analyses.
Get Radiology Tree app to read full this article<
References
1. Lee D.W., Neumann P.J., Rizzo J.A.: Understanding the medical and nonmedical value of diagnostic testing. Value Health 2010; 13: pp. 310-314.
2. Brook R.H.: The RAND/UCLA appropriateness method.McCormick K.A.Moore S.A.Siegel R.A.Methodology perspectives.1994.Public Health Service, U.S. Department of Health and Human ServicesRockville, MD:pp. 59-70.
3. Brook R.H., Chassin M.R., Fink A., et. al.: A method for the detailed assessment of the appropriateness of medical technologies. Int J Technol Assess Health Care 1986; 2: pp. 53-63.
4. Gazelle G.S., Kessler L., Lee D.W., et. al.: A framework for assessing the value of diagnostic imaging in the era of comparative effectiveness research. Radiology 2011; 261: pp. 692-698.
5. Bossuyt P.M., Reitsma J.B., Linnet K., et. al.: Beyond diagnostic accuracy: the clinical utility of diagnostic tests. Clin Chem 2012; 58: pp. 1636-1643.
6. Staub L.P., Dyer S., Lord S.J., et. al.: Linking the evidence: intermediate outcomes in medical test assessments. Int J Technol Assess Health Care 2012; 28: pp. 52-58.
7. Staub L.P., Lord S.J., Simes R.J., et. al.: Using patient management as a surrogate for patient health outcomes in diagnostic test evaluation. BMC Med Res Methodol 2012; 12: pp. 12.
8. Otero H.J., Fang C.H., Sekar M., et. al.: Accuracy, risk and the intrinsic value of diagnostic imaging: a review of the cost-utility literature. Acad Radiol 2012; 19: pp. 599-606.
9. Bossuyt P.M.M., McCaffery K.: Additional patient outcomes and pathways in evaluations of testing.2009.Medical Tests-White Paper SeriesRockville, MD
10. American College of Radiology : About the ACR appropriateness criteria. Available at: http://www.acr.org/Quality-Safety/Appropriateness-Criteria/About-AC Accessed December 11, 2014
11. Rao V.M., Levin D.C.: The overuse of diagnostic imaging and the Choosing Wisely initiative. Ann Intern Med 2012; 157: pp. 574-576.
12. Bresnahan B.W., Garrison L.P.: Diagnostic imaging, economic issues in.2014.ElsevierSan Diego:pp. 189-199.
13. Agapova M., Devine E.B., Bresnahan B.W., et. al.: Applying quantitative benefit-risk analysis to aid regulatory decision making in diagnostic imaging: methods, challenges, and opportunities. Acad Radiol 2014; 21: pp. 1138-1143.
14. FDA : Guidance for industry and Food and Drug Administration staff: factors to consider when making benefit-risk determinations in medical device premarket approval and de novo classifications. Available at: https://www.fda.gov/downloads/medicaldevices/deviceregulationandguidance/guidancedocuments/ucm517504.pdf Accessed March 24, 2017
15. Food and Drug Administration : Patient preference information—submission, review in PMAs, HDE applications, and de novo requests, and inclusion in device labeling. Available at: https://www.fda.gov/downloads/medicaldevices/deviceregulationandguidance/guidancedocuments/ucm446680.pdf Accessed March 24, 2017
16. Agapova M., Bresnahan B.B., Higashi M., et. al.: A proposed approach for quantitative benefit-risk assessment in diagnostic radiology guideline development: the American College of Radiology Appropriateness Criteria Example. J Eval Clin Pract 2017; 23: pp. 128-138.
17. Guest G., MacQueen K.M., Namey E.E.: Applied thematic analysis.2012.Sage PublicationsLos Angeles
18. Fryback D.G., Thornbury J.R.: The efficacy of diagnostic imaging. Med Decis Making 1991; 11: pp. 88-94.
19. Harris P.A., Taylor R., Thielke R., et. al.: Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform 2009; 42: pp. 377-381.
20. Choosing Wisely: An Initiative of ABIM Foundation : Imaging tests for lower-back pain. Available at: http://www.choosingwisely.org/patient-resources/imaging-tests-for-back-pain/ Accessed March 24, 2017
21. Choosing Wisely: An Initiative of ABIM Foundation : Imaging tests for headaches. Available at: http://www.choosingwisely.org/patient-resources/imaging-tests-for-headaches/ Accessed March 24, 2017
22. Mostbeck G., Adam E.J., Nielsen M.B., et. al.: How to diagnose acute appendicitis: ultrasound first. Insights Imaging 2016; 7: pp. 255-263.
23. Westphalen A.C., Hsia R.Y., Maselli J.H., et. al.: Radiological imaging of patients with suspected urinary tract stones: national trends, diagnoses, and predictors. Acad Emerg Med 2011; 18: pp. 699-707.
24. Smith-Bindman R., Aubin C., Bailitz J., et. al.: Ultrasonography versus computed tomography for suspected nephrolithiasis. N Engl J Med 2014; 371: pp. 1100-1110.
25. Hoffmann T.C., Del Mar C.: Patients’ expectations of the benefits and harms of treatments, screening, and tests: a systematic review. JAMA Intern Med 2015; 175: pp. 274-286.
26. ACR Appropriateness Criteria : ACR Appropriateness Criteria® Rating Round Information. Available at: http://www.acr.org/~/media/ACR/Documents/AppCriteria/RatingRoundInfo.pdf Accessed August 4, 2015
27. Schnipper L.E., Davidson N.E., Wollins D.S., et. al.: American Society of Clinical Oncology Statement: a conceptual framework to assess the value of cancer treatment options. J Clin Oncol 2015; 33: pp. 2563-2577.
28. Bossuyt P.M., Reitsma J.B., Bruns D.E., et. al.: Towards complete and accurate reporting of studies of diagnostic accuracy: the STARD initiative. Fam Pract 2004; 21: pp. 4-10.
29. Ferrante di Ruffano L., Hyde C.J., McCaffery K.J., et. al.: Assessing the value of diagnostic tests: a framework for designing and evaluating trials. BMJ 2012; 344: pp. e686.
30. Shekalaghe S., Cancino M., Mavere C., et. al.: Clinical performance of an automated reader in interpreting malaria rapid diagnostic tests in Tanzania. Malar J 2013; 12: pp. 141.
31. Novielli N., Cooper N.J., Sutton A.J.: Evaluating the cost-effectiveness of diagnostic tests in combination: is it important to allow for performance dependency?. Value Health 2013; 16: pp. 536-541.
32. Batwala V., Magnussen P., Nuwaha F.: Comparative feasibility of implementing rapid diagnostic test and microscopy for parasitological diagnosis of malaria in Uganda. Malar J 2011; 10: pp. 373.
33. Fowler J.R., Maltenfort M.G., Ilyas A.M.: Ultrasound as a first-line test in the diagnosis of carpal tunnel syndrome: a cost-effectiveness analysis. Clin Orthop Relat Res 2013; 471: pp. 932-937.
34. Freixa X., Trilla M., Feldman M., et. al.: Right versus left transradial approach for coronary catheterization in octogenarian patients. Catheter Cardiovasc Interv 2012; 80: pp. 267-272.
35. Pulcini C., Pauvif L., Paraponaris A., et. al.: Perceptions and attitudes of French general practitioners towards rapid antigen diagnostic tests in acute pharyngitis using a randomized case vignette study. J Antimicrob Chemother 2012; 67: pp. 1540-1546.
36. Rossi I.A., D’Acremont V., Prod’Hom G., et. al.: Safety of falciparum malaria diagnostic strategy based on rapid diagnostic tests in returning travellers and migrants: a retrospective study. Malar J 2012; 11: pp. 377.
37. Loganathan A.G., Chan M.D., Alphonse N., et. al.: Clinical outcomes of brain metastases treated with Gamma Knife radiosurgery with 3.0 T versus 1.5 T MRI-based treatment planning: have we finally optimised detection of occult brain metastases?. J Med Imaging Radiat Oncol 2012; 56: pp. 554-560.
38. Than M., Cullen L., Aldous S., et. al.: 2-Hour accelerated diagnostic protocol to assess patients with chest pain symptoms using contemporary troponins as the only biomarker: the ADAPT trial. J Am Coll Cardiol 2012; 59: pp. 2091-2098.
39. Margolis N.E., Shaver C.M., Rosenkrantz A.B.: Indeterminate liver and renal lesions: comparison of computed tomography and magnetic resonance imaging in providing a definitive diagnosis and impact on recommendations for additional imaging. J Comput Assist Tomogr 2013; 37: pp. 882-886.
40. Rodrigo E., Lopez-Hoyos M., Corral M., et. al.: ImmuKnow as a diagnostic tool for predicting infection and acute rejection in adult liver transplant recipients: a systematic review and meta-analysis. Liver Transpl 2012; 18: pp. 1245-1253.
41. Beaton A., Okello E., Lwabi P., et. al.: Echocardiography screening for rheumatic heart disease in Ugandan schoolchildren. Circulation 2012; 125: pp. 3127-3132.
42. Simprini L.A., Taylor A.J.: Cardiac CT in women: clinical application and considerations. J Cardiovasc Comput Tomogr 2012; 6: pp. 71-77.
43. Moschetti K., Muzzarelli S., Pinget C., et. al.: Cost evaluation of cardiovascular magnetic resonance versus coronary angiography for the diagnostic work-up of coronary artery disease: application of the European Cardiovascular Magnetic Resonance registry data to the German, United Kingdom, Swiss, and United States health care systems. J Cardiovasc Magn Reson 2012; 14: pp. 35.
44. Nance J.W., Bamberg F., Schoepf U.J.: Coronary computed tomography angiography in patients with chronic chest pain: systematic review of evidence base and cost-effectiveness. J Thorac Imaging 2012; 27: pp. 277-288.
45. Wagner J., Aron D.C.: Incidentalomas: a “disease” of modern imaging technology. Best Pract Res Clin Endocrinol Metab 2012; 26: pp. 3-8.
46. Tagliafico A., Succio G., Serafini G., et. al.: Diagnostic performance of ultrasound in patients with suspected brachial plexus lesions in adults: a multicenter retrospective study with MRI, surgical findings and clinical follow-up as reference standard. Skeletal Radiol 2013; 42: pp. 371-376.
47. Azeem N., Tabibian J.H., Baron T.H., et. al.: Use of a single-balloon enteroscope compared with variable-stiffness colonoscopes for endoscopic retrograde cholangiography in liver transplant patients with Roux-en-Y biliary anastomosis. Gastrointest Endosc 2013; 77: pp. 568-577.
48. Spencer J.D., Bates C.M., Mahan J.D., et. al.: The accuracy and health risks of a voiding cystourethrogram after a febrile urinary tract infection. J Pediatr Urol 2012; 8: pp. 72-76.
49. von Wagner C., Ghanouni A., Halligan S., et. al.: Patient acceptability and psychologic consequences of CT colonography compared with those of colonoscopy: results from a multicenter randomized controlled trial of symptomatic patients. Radiology 2012; 263: pp. 723-731.
50. Mudrick D.W., Cowper P.A., Shah B.R., et. al.: Downstream procedures and outcomes after stress testing for chest pain without known coronary artery disease in the United States. Am Heart J 2012; 163: pp. 454-461.
51. Ma S., Kong B., Liu B., et. al.: Biological effects of low-dose radiation from computed tomography scanning. Int J Radiat Biol 2013; 89: pp. 326-333.
52. Lin Y.K., Gettle L., Raman J.D.: Significant variability in 10-year cumulative radiation exposure incurred on different surveillance regimens after surgery for pT1 renal cancers: yet another reason to standardize protocols?. BJU Int 2013; 111: pp. 891-896.
53. Hao R., Zhang Q., Xu Z., et. al.: Magnetic navigation system and CT roadmap-assisted percutaneous coronary intervention: a comparison to the conventional approach. J Invasive Cardiol 2013; 25: pp. 177-181.
54. Shahbazi-Gahrouei D., Baradaran-Ghahfarokhi M.: Assessment of entrance surface dose and health risk from common radiology examinations in Iran. Radiat Prot Dosimetry 2013; 154: pp. 308-313.
55. Martin C.J., Huda W.: Intercomparison of patient CTDI surveys in three countries. Radiat Prot Dosimetry 2013; 153: pp. 431-440.
56. Shah D.J., Sachs R.K., Wilson D.J.: Radiation-induced cancer: a modern view. Br J Radiol 2012; 85: pp. e1166-e1173.
57. Smith I.R., Cameron J., Mengersen K.L., et. al.: Evaluation of coronary angiographic projections to balance the clinical yield with the radiation risk. Br J Radiol 2012; 85: pp. e722-e728.
58. Norgaz T., Gorgulu S., Dagdelen S.: A randomized study comparing the effectiveness of right and left radial approach for coronary angiography. Catheter Cardiovasc Interv 2012; 80: pp. 260-264.
59. Durand D.J., Dixon R.L., Morin R.L.: Utilization strategies for cumulative dose estimates: a review and rational assessment. J Am Coll Radiol 2012; 9: pp. 480-485.
60. Koshy S., Thompson R.C.: Review of radiation reduction strategies in clinical cardiovascular imaging. Cardiol Rev 2012; 20: pp. 139-144.
61. Kusmierek J., Plachcinska A.: Patient exposure to ionising radiation due to nuclear medicine cardiac procedures. Nucl Med Rev Cent East Eur 2012; 15: pp. 71-74.
62. Grunheid T., Kolbeck Schieck J.R., Pliska B.T., et. al.: Dosimetry of a cone-beam computed tomography machine compared with a digital x-ray machine in orthodontic imaging. Am J Orthod Dentofacial Orthop 2012; 141: pp. 436-443.
63. van Vlijmen O.J., Kuijpers M.A., Berge S.J., et. al.: Evidence supporting the use of cone-beam computed tomography in orthodontics. J Am Dent Assoc 2012; 143: pp. 241-252.
64. Barrett B., Stiles M., Patterson J.: Radiation risks: critical analysis and commentary. Prev Med 2012; 54: pp. 280-282.
65. Schoenhagen P., Thompson C.M., Halliburton S.S.: Low-dose cardiovascular computed tomography: where are the limits?. Curr Cardiol Rep 2012; 14: pp. 17-23.
66. Ewer A.K., Furmston A.T., Middleton L.J., et. al.: Pulse oximetry as a screening test for congenital heart defects in newborn infants: a test accuracy study with evaluation of acceptability and cost-effectiveness. Health Technol Assess 2012; 16: pp. v-xiii. 1-184
67. Fennich N., Ellouali F., Abdelali S., et. al.: Stress echocardiography: safety and tolerability. Cardiovasc Ultrasound 2013; 11: pp. 30.
68. Winer J.L., Liu C.Y., Apuzzo M.L.: The use of nanoparticles as contrast media in neuroimaging: a statement on toxicity. World Neurosurg 2012; 78: pp. 709-711.
69. Firouzi A., Eshraghi A., Shakerian F., et. al.: Efficacy of pentoxifylline in prevention of contrast-induced nephropathy in angioplasty patients. Int Urol Nephrol 2012; 44: pp. 1145-1149.
70. Neubauer A., Wolfsberger S.: Virtual endoscopy in neurosurgery: a review. Neurosurgery 2013; 72: pp. 97-106.
71. Tay C.M., Chang S.K.: Diagnosis and management of pancreaticopleural fistula. Singapore Med J 2013; 54: pp. 190-194.
72. Jenssen C., Alvarez-Sanchez M.V., Napoleon B., et. al.: Diagnostic endoscopic ultrasonography: assessment of safety and prevention of complications. World J Gastroenterol 2012; 18: pp. 4659-4676.
73. Pinto S., Pinto A., de Carvalho M.: Phrenic nerve studies predict survival in amyotrophic lateral sclerosis. Clin Neurophysiol 2012; 123: pp. 2454-2459.
74. Zondervan R.L., Hahn P.F., Sadow C.A., et. al.: Body CT scanning in young adults: examination indications, patient outcomes, and risk of radiation-induced cancer. Radiology 2013; 267: pp. 460-469.
75. Hilgerink M.P., Hummel M.J., Manohar S., et. al.: Assessment of the added value of the Twente Photoacoustic Mammoscope in breast cancer diagnosis. Med Devices (Auckl) 2011; 4: pp. 107-115.
76. Do CT scans cause cancer? For older men the risk from diagnostic CT scans is relatively small. Harv Mens Health Watch 2013; 17: pp. 3.
77. Krille L., Zeeb H., Jahnen A., et. al.: Computed tomographies and cancer risk in children: a literature overview of CT practices, risk estimations and an epidemiologic cohort study proposal. Radiat Environ Biophys 2012; 51: pp. 103-111.
78. Pauwels E.K., Bourguignon M.H.: Radiation dose features and solid cancer induction in pediatric computed tomography. Med Princ Pract 2012; 21: pp. 508-515.
79. Saltzherr T.P., Goslings J.C., Bakker F.C., et. al.: Cost-effectiveness of trauma CT in the trauma room versus the radiology department: the REACT trial. Eur Radiol 2013; 23: pp. 148-155.
80. Zheng D., Huang X., Fan Y., et. al.: The effect of octreotide treatment on patients with pancreatic cancer who undergo endoscopic retrograde cholangiopancreatography (ERCP) with pancreatic duct stent placement. Hepatogastroenterology 2013; 60: pp. 222-224.