
Rationale and Objectives
To evaluate the efficacy of a self-expanding metal stent seeded with autologous endothelial progenitor cells (EPCs) for preventing in-stent stenoses in transjugular intrahepatic portosystemic shunt (TIPS) in a swine model.
Materials and Methods
TIPS was performed in 18 young adult pigs, using a self-expanding nitinol stent (control, n = 8) and an autologous EPC-seeded stent (treatment, n = 10). All pigs were sacrificed at 2 weeks post-TIPS procedure. Portography was performed immediately before the euthanasia. Gross, microscopic, and immunohistochemistry of the TIPS tract specimens were examined. The proliferative response of the shunt was quantified histologically.
Results
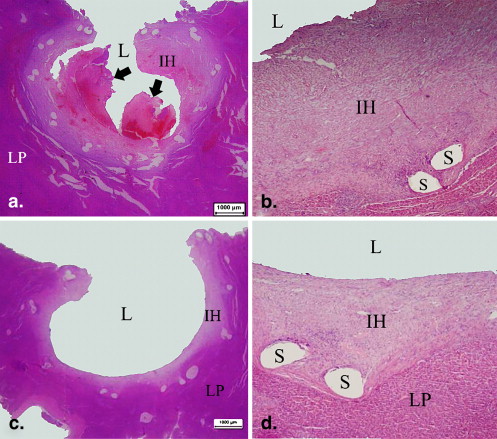
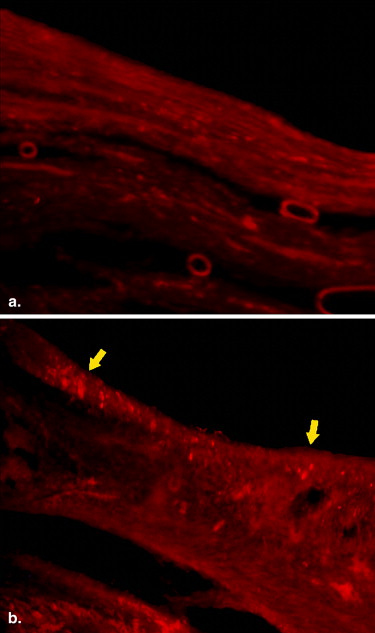
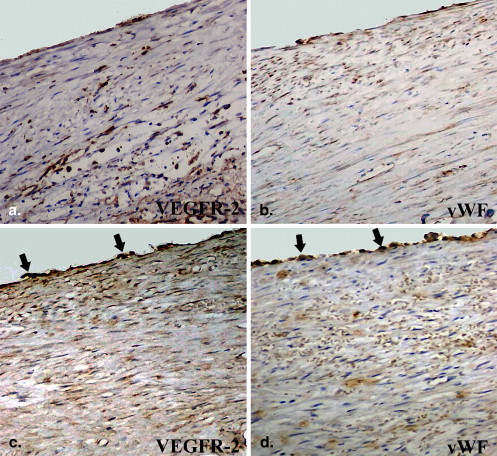
TIPS was performed successfully in 16 swine, 2 animals died during the procedure. Another pig died of unknown causes 2 days post-procedure. At day 14 follow-up, portography and necropsy of the 15 remaining swine demonstrated that five shunts occluded and one shunt was stenotic (80%) in the control group ( n = 6). Five shunts remained patent, two shunts were stenosed (50%, 70%), and the remaining two shunts were occluded in the treatment group ( n = 9). The patency rate was significantly lower in the control group than in the treatment group, 0% versus 55.6% ( P = .03). Histological analyses showed a significantly greater pseudointimal hyperplasia in the TIPS track of the control group than that of the treatment group ( P < .05). Intact endothelium was documented in the lumina of all the EPC-implanted stent group.
Conclusions
The EPC-seeded metal stent is feasibly fabricated in vitro and improves the patency in TIPS in a porcine model.
Transjugular intrahepatic portosystemic shunt (TIPS) has been in use for more than 20 years to treat recurrent variceal hemorrhage and refractory ascites caused by portal hypertension . However, shunt stenosis or occlusion remains a major obstacle to the utility of TIPS . Several investigators have suggested that bile leakage is inevitable during a TIPS procedure and there may be small bile ducts in communication with the TIPS tract that may account for the neointimal overgrowth . Bile leak inhibits smooth muscle cell proliferation instead of promoting their growth in an in vitro cell culture, and further study shows that such bile leakage may promote in-stent stenosis in a TIPS shunt by inhibiting endothelial cell proliferation . Using a physical barrier to block bile and cytokine leakage between the circulation and the injured hepatic parenchyma has been shown to prevent in-stent stenosis of TIPS . Another potential method to prevent in-stent stenosis is the induction of rapid endogenous reendothelialization of the tract to inhibit the bile leakage that is associated with early stage thrombosis and late stage pseudointimal overgrowth within a TIPS shunt . The design of an autologous endothelialized stent graft to prevent post-TIPS in-stent stenosis holds great promise. Although Zhuang showed that the TIPS shunt patency improves significantly at 2 weeks in a swine model with an autologous vein-covered stent, such a technique does not seem practical in routine clinical use.
It is known that endothelial progenitor cells (EPCs) can differentiate into endothelial cells in vivo and can easily be harvested from peripheral blood . In this study, we designed a novel endoprosthesis for TIPS that was seeded with autologous EPCs to test that the shunt patency would be improved with this device when compared with a bare metal self-expanding stent.
Materials and methods
Get Radiology Tree app to read full this article<
Preparation of EPC-seeded Stent
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TIPS Creation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Follow-up
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
EPC-seeded Stent Fabrication in vitro
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TIPS Procedure
Get Radiology Tree app to read full this article<
Follow-up Portography and Histopathology
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Results of the TIPS Creation in a Swine Model with Bare or EPC-seeded Stent
Animal No. Gender Weight (kg) Stent Type Follow-up Duration Tract Status 1 F 20 Bare 14 Occlusion 2 F 30 EPC-seeded 15 Occlusion 3 M 25 Bare 15 Occlusion 4 M 25 EPC-seeded 14 Patent 5 F 32 EPC-seeded 14 Stenosis 50% 6 F 25 EPC-seeded 14 Occlusion 7 F 20 EPC-seeded 13 Patent 8 F 20 Bare 14 Occlusion 9 F 20 Bare 14 Occlusion 10 F 20 EPC-seeded 14 Stenosis 70% 11 ∗ F 25 Bare 2 Stenosis 60% 12 M 25 EPC-seeded 15 Patent 13 M 25 EPC-seeded 14 Patent 14 F 23 EPC-seeded 13 Patent 15 M 25 Bare 15 Stenosis 80% 16 F 20 Bare 14 Occlusion
F, female; M, male; bare, bare metal stent; EPC-seeded, endothelial progenitor cell–seeded metal stent with fibrin gel.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Morphometry Analysis of the TIPS Shunts
PIH Area (mm 2 ) PIH Thickness(mm) Sites Bare Stent EPC-seeded Bare Stent EPC-seeded Hepatic vein segment 14.3 ± 6.53 11.1 ± 5.66 1.20 ± 0.37 0.97 ± 0.56 ∗ Central segment 12.0 ± 4.57 9.68 ± 5.46 ∗ 1.26 ± 0.45 0.85 ± 0.47 ∗ Portal vein segment 12.1 ± 5.56 10.5 ± 5.2 1.50 ± 0.36 0.98 ± 0.44 ∗
PIH, pseudointimal hyperplasia; PIH thickness, distance from the stent wires to lumen; TIPS, transjugular intrahepatic portosystemic shunt.
PIH area not including thrombus.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgment
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Richter G.M., Noeldge G., Palmaz J.C., et. al.: Transjugular intrahepatic portosystemic shunt: preliminary clinical results. Radiology 1990; 174: pp. 1027-1030.
2. Coldwell D.M., Ring E.J., Rees C.R., et. al.: Multicenter investigation of the role of transjugular intrahepatic portosystemic shunt in management of portal hypertension. Radiology 1995; 196: pp. 335-340.
3. Zhuang Z.W., Teng G.J., Jeffery R.F., et. al.: Long-term results and quality of life in patients treated with transjugular intrahepatic portosystemic shunts. Am J Roentgenol 2002; 179: pp. 1597-1603.
4. LaBerge J.M., Ferrell L.D., Ring E.J., et. al.: Histologic study of stenotic and occluded transjugular intrahepatic portosystemic shunts. J Vasc Interv Radiol 1993; 4: pp. 779-786.
5. Saxon R.R., Mende-Hartvig J., Corless C.L., et. al.: Bile duct injury as a major cause of stenosis and occlusion in transjugular intrahepatic portosystemic shunts: comparative histopathologic analysis in humans and swine. J Vasc Interv Radiol 1996; 7: pp. 487-497.
6. Teng G.J., Bettmann M.A., Hoopes P.J., et. al.: Transjugular intrahepatic portosystemic shunt: effect of bile leak on smooth muscle cell proliferation. Radiology 1998; 208: pp. 799-805.
7. Teng G.J., Lu Q.: Bile leakage during transjugular intrahepatic portosystemic shunt creation: in vitro effect of bile on growth and function of human umbilical vein endothelium. Radiology 2005; 235: pp. 867-871.
8. Cejna M., Thurnher S., Pidlich J., et. al.: Primary implantation of polyester-covered stent-grafts for transjugular intrahepatic portosystemic stent shunts (TIPSS): a pilot study. Cardio Vasc Interv Radiol 1999; 22: pp. 305-310.
9. Cejna M., Peck-Radosavljevic M., Thurnher S.A., et. al.: Creation of transjugular intrahepatic portosystemic shunts with stent-grafts: initial experiences with a polytetrafluoroethylene covered nitinol endoprosthesis. Radiology 2001; 221: pp. 437-446.
10. Hausegger K.A., Karnel F., Georgieva B., et. al.: Transjugular intrahepatic portosystemic shunt creation with the Viatorr expanded polytetrafluoroethylene-covered stent-graft. J Vasc Interv Radiol 2004; 15: pp. 239-248.
11. Vignali C., Bargellini I., Grosso M., et. al.: TIPS with expanded polytetrafluoroethylene-covered stent: results of an Italian multicenter study. Am J Roentgenol 2005; 185: pp. 472-480.
12. Murad S.D., Luong T.K., Pattynama P.M.T., et. al.: Long-term outcome of a covered vs. uncovered transjugular intrahepatic portosystemic shunt in Budd-Chiari syndrome. Liver Int 2008; 28: pp. 249-256.
13. Zhuang Z.W., Hoopes P.J., Koutras P.C., et. al.: Transjugular intrahepatic portosystemic shunt with an autologous vein-covered stent: results in a swine model. J Vasc Interv Radiol 2001; 12: pp. 1333-1342.
14. Asahara T., Murohara T., Sullivan A., et. al.: Isolation of putative progenitor endothelial cells for angiogenesis. Science 1997; 275: pp. 964-967.
15. Werner N., Junk S., Laufs U., et. al.: Intravenous transfusion of endothelial progenitor cells reduces neointima formation after vascular injury. Circ Res 2003; 93: pp. e17-e24.
16. Depalma L., Criss V.R., Luban N.L.C.: The preparation of fibrinogen concentrate for use as fibrin glue by four different methods. Transfusion 1993; 33: pp. 717-720.
17. Kipshidze N., Ferguson J., Keelan M.H., et. al.: Endoluminal reconstruction of the arterial wall with endothelial cell/glue matrix reduces restenosis in an atherosclerotic rabbit. J Am Coll Cardiol 2000; 36: pp. 1396-1403.
18. Teng G.J., Bettmann M.A., Hoopes P.J., et. al.: Transjugular intrahepatic portosystemic shunt in a porcine model: histologic characteristic at the early stage. Acad Radiol 1998; 5: pp. 547-555.
19. Contos M.J., Kornstein M.J., Innes D.J., et. al.: The utility of CD20 and CD43 in subclassification of low-grade B-cell lymphoma on paraffin sections. Mod Pathol 1992; 5: pp. 631-633.
20. Haskal Z.J.: Improved patency of transjugular intrahepatic portosystemic shunts in humans: creation and revision with PTFE stent-grafts. Radiology 1999; 213: pp. 759-766.
21. Ben-Shoshan J., George J.: Endothelial progenitor cells as therapeutic vectors in cardiovascular disorders: from experimental models to human trials. Pharmacol Therapeutics 2007; 15: pp. 25-36.
22. Gines P., Cardenas A., Arroyo V., et. al.: Management of cirrhosis and ascites. N Engl J Med 2004; 350: pp. 1646-1653.
23. Boyer T.D., Haskal Z.J.: The role of transjugular intrahepatic portosystemic shunt in the management of portal hypertension. Hepatology 2005; 41: pp. 386-400.
24. Salerno F., Camma C., Enea M., et. al.: Transjugular intrahepatic portosystemic shunt for refractory ascites: a meta-analysis of individual patient data. Gastroenterology 2007; 133: pp. 825-884.
25. Boyer T.D., Henderson J.M., Heerey A.M., et. al.: Cost of preventing variceal rebleeding with transjugular intrahepatic portal systemic shunt and distal splenorenal shunt. J Hepatol 2008; 48: pp. 407-414.
26. Barrioa J., Ripolla C., Banaresa R., et. al.: Comparison of transjugular intrahepatic portosystemic shunt dysfunction in PTFE-covered stent-grafts versus bare stents. Eur J Radiol 2005; 55: pp. 120-124.
27. Gandini R., Konda D., Simonetti G.: Transjugular intrahepatic portosystemic shunt patency and clinical outcome in patients with Budd-Chiari syndrome: covered versus uncovered stents. Radiology 2006; 241: pp. 298-305.
28. Tripathi D., Ferguson J., Barkell H., et. al.: Improved clinical outcome with transjugular intrahepatic portosystemic stent-shunt utilizing polytetrafluoroethylene-covered stents. Eur J Gastroenterol Hepatol 2006; 18: pp. 225-232.
29. Ferguson W., Tripathi D., Redhead D.N., et. al.: Transient segmental liver ischaemia after polytetrafluoroethylene transjugular intrahepatic portosystemic stent-shunt procedure. J Hepatol 2005; 42: pp. 145.
30. Serruys P.W., Kutryk M.J.B., Ong A.T.L.: Coronary stents. N Engl J Med 2006; 354: pp. 483-495.
31. Bhattacharya V., McSweeney P.A., Shi Q., et. al.: Enhanced endothelialization and microvessel formation in polyester grafts seeded with CD 34+ bone marrow cells. Blood 2000; 95: pp. 581-585.
32. Griese D., Ehsan A., Melo L.G., et. al.: Isolation and transplantation of autologous circulating endothelial cells into denuded vessels and prosthetic grafts: implications for cell-based vascular therapy. Circulation 2003; 108: pp. 2710-2715.
33. Inoue T., Sata M., Hikichi Y., et. al.: Mobilization of CD34-positive bone marrow-derived cells after coronary stent implantation: impact on restenosis. Circulation 2007; 115: pp. 553-561.
34. Walter D.K., Cejna M., Diaz-Sandoval L., et. al.: Local gene transfer of phVEGF-2 plasmid by gene-eluting stents: an alternative strategy for inhibition of restenosis. Circulation 2004; 110: pp. 36-45.
35. Aoki J., Serruys P.W., van Beusekom H., et. al.: Endothelial progenitor cell capture by stents coated with antibody against CD34: the HEALING-FIM (Healthy Endothelial Accelerate Lining Inhibits Neointimal Growth-First In Man). Registry. J Am Coll Cardiol 2005; 45: pp. 1574-1579.
36. Yu X., Wan C., Chen H.: Preparation and endothelialization of decellularised vascular scaffold for tissue-engineered blood vessel. J Mater Sci Mater Med 2008; 19: pp. 319-326.
37. Conte M.S., VanMeter G.A., Akst L.M., et. al.: Endothelial cell seeding influences lesion development following arterial injury in the cholesterol-fed rabbit. Cardiovasc Res 2002; 53: pp. 502-511.
38. Shirota T., Yasui H., Shimokawa H., et. al.: Fabrication of endothelial progenitor cell (EPC)-seeded intravascular stent devices and in vitro endothelialization on hybrid vascular tissue. Biomaterials 2003; 24: pp. 2295-2302.
39. Sanyal A.J., Mirshahi F.: Endothelial cells lining transjugular intrahepatic portasystemic shunts originate in hepatic sinusoids: implications for pseudointimal hyperplasia. Hepatology 1999; 29: pp. 710-718.
40. Egashira K., Nakano K., Ohtani K., et. al.: Local delivery of anti-monocyte chemoattractant protein-1 by gene-eluting stents attenuates in-stent stenosis in rabbits and monkeys. Arterioscler Thromb Vasc Biol 2007; 27: pp. 2563-2568.
41. Sharif F., Hynes S.O., Cooney R., et. al.: Gene-eluting stents: adenovirus-mediated delivery of Enos to the blood vessels wall accelerates re-endothelialization and inhibits restenosis. Mol Ther 2008; 16: pp. 1674-1680.
42. Matsumoto Y., Adams V., Walther C., et. al.: Reduced number and function of endothelial progenitor cells in patients with aortic valve stenosis: a novel concept for valvular endothelial cell repair. Eur Heart J 2009; 30: pp. 346-355.
43. Nowak G., Karrar A., Holmen C., et. al.: Expression of vascular endothelial growth factor receptor-2 or Tie-2 on peripheral blood cells defines functionally competent cell populations capable of reendothelialization. Circulation 2004; 110: pp. 3699-3707.
44. Sanyal A.J., Contos M.J., Yager D., et. al.: Development of pseudointima and stenosis after transjugular intrahepatic portasystemic shunts: characterization of cell phenotype and function. Hepatology 1998; 28: pp. 22-32.
45. Haskal Z.J., Brennecke L.H.: Transjugular intrahepatic portosystemic shunts formed with polyethylene terephthalate-covered stents: experimental evaluation in pigs. Radiology 1999; 213: pp. 853-859.