
Rationale and Objectives
Several studies have shown that multislice computed tomography (MSCT) has a high sensitivity and specificity for detecting coronary artery stenoses. The aim of the present study was to investigate whether MSCT can reliably triage patients with suspected coronary artery disease (CAD) to coronary artery bypass grafting (CABG), percutaneous coronary intervention (PCI), or no revascularization.
Materials and Methods
A total of 123 patients with suspected CAD who were referred for conventional coronary angiography (CATH) additionally underwent MSCT (16*0.5 mm detector collimation). Therapeutic decisions made on the basis of CATH and MSCT strictly following current guidelines for treatment of CAD were compared with decisions made by a cardiac surgeon and an interventional cardiologist. Only MSCTs with at least adequate image quality in all coronary segments were included in the analysis (94/123).
Results
Decisions made on the basis of MSCT and CATH according to guidelines did not differ significantly (agreement of 88%, 82 of 94, P = .319). The therapeutic decisions made by the interventional cardiologist and the cardiac surgeon based on CATH differed significantly (overall agreement of 79%, 74 of 94 cases, P < .001; cardiologist: 78% PCI and 22% CABG versus surgeon: 38% PCI and 62% CABG), whereas there was 100% agreement regarding decisions for or against invasive treatment.
Conclusions
MSCT shows good agreement with CATH in triaging patients with suspected CAD to CABG, PCI, or no revascularization. The choice of revascularization procedure is significantly more strongly influenced by whether an interventional cardiologist or a cardiac surgeon makes the decision than by the diagnostic test on which the decision is based.
Coronary artery disease (CAD) is one of the most common diseases in industrialized countries ( ). It is diagnosed noninvasively using resting electrocardiography (ECG), exercise ECG, scintigraphy, echocardiography, and stress echocardiography. These diagnostic tests vary in their sensitivities and specificities ( ). CAD is confirmed or excluded invasively by conventional coronary angiography (CATH), which has a mortality of 0.11% and a complication rate of 1.7% for major adverse cardiac and cerebrovascular events (MACCE) when performed as an elective diagnostic procedure ( ). Multislice computed tomography (MSCT) involves the same radiation exposure and reliably depicts the coronary vessels with a sensitivity and specificity for the detection of hemodynamically significant stenoses of 85% and 95%, respectively. The technical advances made in recent years have continuously improved image analysis ( ). The aim of the present study was to determine how well a therapeutic decision for either coronary artery bypass grafting (CABG), percutaneous coronary intervention (PCI), or no revascularization can be made on the basis of the MSCT findings in comparison with CATH (gold standard). To this end, we compared the therapeutic decisions made on the basis of MSCT and CATH in accordance with current guidelines with the therapeutic decisions made by specialists for PCI (interventional cardiologist) and CABG (cardiac surgeon).
Material and methods
Patients
One hundred and twenty-three (92 men and 31 women, mean age 62.3 ± 8.7 years) with suspected CAD who were referred to our institution by outpatient centers were investigated by elective CATH and MSCT as part of an investigator-initiated study comparing MSCT and magnetic resonance coronary angiography ( ). Inclusion criteria were age at least 40 years and a sinus rhythm. Patients with contraindications to iodinated contrast agents, renal insufficiency, cardiac arrhythmia, coronary artery stents, or bypass grafts were excluded. The study was approved by the institutional review board and all patients gave written informed consent.
MSCT Protocol
Get Radiology Tree app to read full this article<
Conventional Coronary Angiography
Get Radiology Tree app to read full this article<
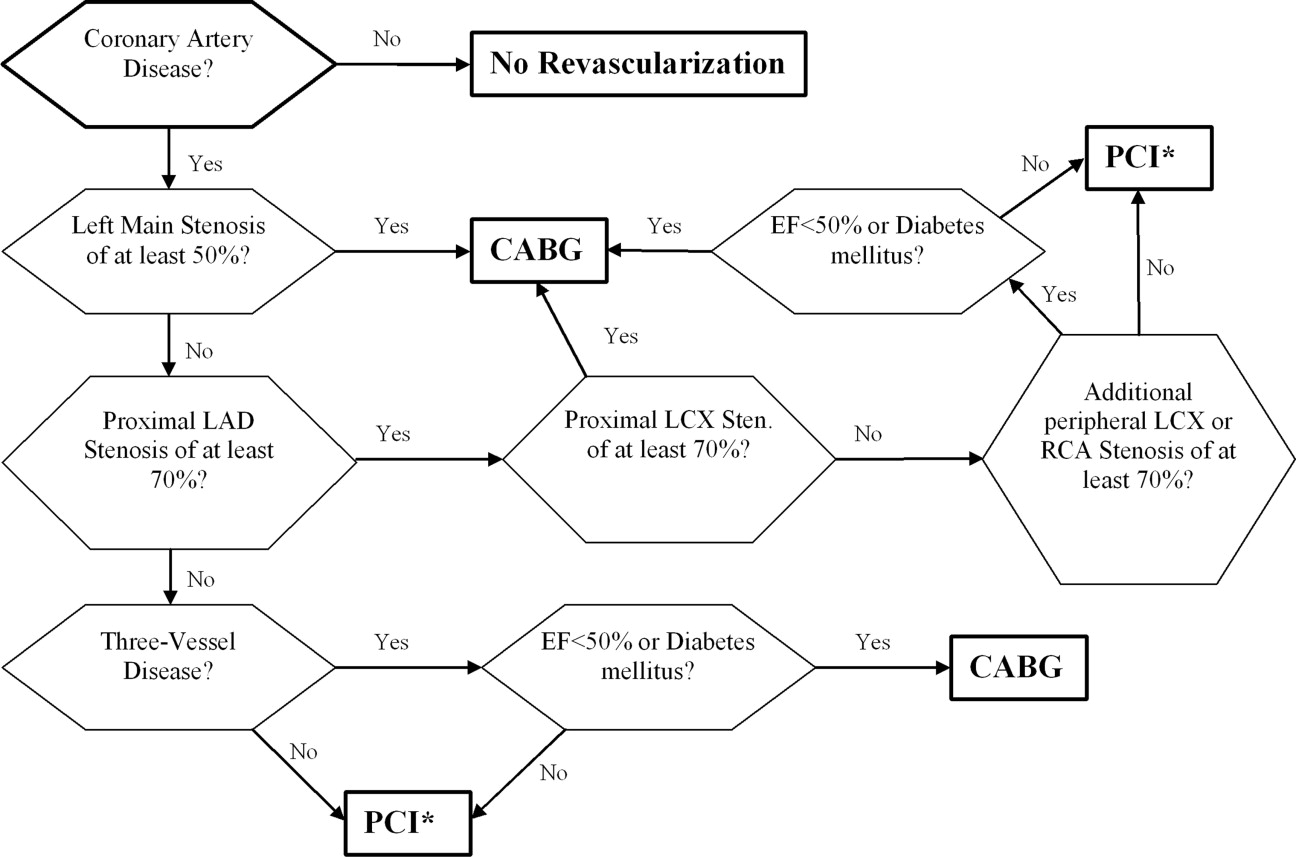
Guideline-Based Triage Using a Flow Chart
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Therapeutic Decision-Making by an Interventional Cardiologist and a Cardiac Surgeon
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 1
Agreement of Therapeutic Decisions Based on MSCT and CATH Made According to the Guidelines for the Treatment of Coronary Artery Disease
MSCT CABG PCI No Revascularization Total CATH CABG 9 1 0 10 PCI 3 27 5 35 No revascularization 0 2 47 49 Total 12 30 52 94
The statistical results were as follows: agreement: 88%; Kappa: 0.798; McNemar’s test: P = .319; agreement for decision between PCI and CABG: 90%; agreement for decision between revascularization and no revascularization: 93%; accuracy for decision for revascularization: 89%; accuracy for decision against revascularization: 96%; predictive value of MSCT for revascularization: 95%.
CABG: coronary artery bypass graft; CATH: conventional coronary angiography; MSCT: multislice computed tomography; PCI: percutaneous coronary intervention.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Agreement Between Interventional Cardiologist and Cardiac Surgeon Based on CATH
Cardiac Surgeon CABG PCI No Revascularization Total Interventional cardiologist CABG 11 0 0 11 PCI 20 19 0 39 No revascularization 0 0 44 44 Total 31 19 44 94
The statistical results were as follows: agreement: 79%; McNemar’s: P < .001 (indicating significant differences between the two physicians); Kappa: 0.677; agreement for decision between PCI and CABG: 60%; and agreement for decision between revascularization and no revascularization: 100%.
CABG: coronary artery bypass graft; CATH: conventional coronary angiography; MSCT: multislice computed tomography; PCI: percutaneous coronary intervention.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Agreement Between Interventional Cardiologist and Cardiac Surgeon Based on MSCT
Cardiac Surgeon CABG PCI No Revascularization Total Interventional cardiologist CABG 6 0 0 6 PCI 21 17 0 38 No revascularization 0 1 49 50 Total 27 18 49 94
The statistical results were as follows: agreement: 77%; McNemar’s test: P < .001 (indicating significant differences between the two physicians); Kappa: 0.672; agreement for decision between PCI and CABG: 52%; and agreement for decision between revascularization and no revascularization: 99%.
CABG: coronary artery bypass graft; CATH: conventional coronary angiography; MSCT: multislice computed tomography; PCI: percutaneous coronary intervention.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Tunstall-Pedoe H., Kuulasmaa K., Mahonen M., et. al.: Contribution of trends in survival and coronary-event rates to changes in coronary heart disease mortality: 10-year results from 37 WHO MONICA project populations. Lancet 1999; 353: pp. 1547-1557.
2. Dewey M., Richter W.S., Lembcke A., et. al.: Noninvasive diagnosis of coronary artery disease. Med Klin 2004; 99: pp. 57-64. (Munich)
3. Noto T.J., Johnson L.W., Krone R., et. al.: Cardiac catheterization 1990: a report of the Registry of the Society for Cardiac Angiography and Interventions (SCA&I). Cathet Cardiovasc Diagn 1991; 24: pp. 75-83.
4. Garcia M.J., Lessick J., Hoffmann M.H.: Accuracy of 16-row multidetector computed tomography for the assessment of coronary artery stenosis. JAMA 2006; 296: pp. 403-411.
5. Schuijf J.D., Bax J.J., Shaw L.J., et. al.: Meta-analysis of comparative diagnostic performance of magnetic resonance imaging and multislice computed tomography for noninvasive coronary angiography. Am Heart J 2006; 151: pp. 404-411.
6. Dewey M., Teige F., Schnapauff D., et. al.: Noninvasive detection of coronary artery stenoses with multislice computed tomography or magnetic resonance imaging. Ann Intern Med 2006; 145: pp. 407-415.
7. Austen W.G., Edwards J.E., Frye R.L., et. al.: A reporting system on patients evaluated for coronary artery disease. Circulation 1975; 51: pp. 5-40.
8. Knottnerus J.A., Muris J.W.: Assessment of the accuracy of diagnostic tests: the cross-sectional study. J Clin Epidemiol 2003; 56: pp. 1118-1128.
9. Gibbons R.J., Abrams J., Chatterjee K., et. al.: ACC/AHA 2002 guideline update for the management of patients with chronic stable angina—summary article: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on the Management of Patients With Chronic Stable Angina). Circulation 2003; 107: pp. 149-158.
10. Smith S.C., Dove J.T., Jacobs A.K., et. al.: ACC/AHA guidelines for percutaneous coronary intervention (revision of the 1993 PTCA guidelines)—executive summary: a report of the American College of Cardiology/American Heart Association task force on practice guidelines (Committee to revise the 1993 guidelines for percutaneous transluminal coronary angioplasty) endorsed by the Society for Cardiac Angiography and Interventions. Circulation 2001; 103: pp. 3019-3041.
11. Eagle K.A., Guyton R.A., Davidoff R., et. al.: ACC/AHA 2004 guideline update for coronary artery bypass graft surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Update the 1999 Guidelines for Coronary Artery Bypass Graft Surgery). Circulation 2004; 110: pp. e340-e437.
12. Mollet N.R., Cademartiri F., Krestin G.P., et. al.: Improved diagnostic accuracy with 16-row multi-slice computed tomography coronary angiography. J Am Coll Cardiol 2005; 45: pp. 128-132.
13. Leschka S., Alkadhi H., Plass A., et. al.: Accuracy of MSCT coronary angiography with 64-slice technology: first experience. Eur Heart J 2005; 26: pp. 1482-1487.
14. Leber A.W., Knez A., von Ziegler F., et. al.: Quantification of obstructive and nonobstructive coronary lesions by 64-slice computed tomography: a comparative study with quantitative coronary angiography and intravascular ultrasound. J Am Coll Cardiol 2005; 46: pp. 147-154.
15. Raff G.L., Gallagher M.J., O’Neill W.W., et. al.: Diagnostic accuracy of noninvasive coronary angiography using 64-slice spiral computed tomography. J Am Coll Cardiol 2005; 46: pp. 552-557.
16. Pugliese F., Mollet N.R., Runza G., et. al.: Diagnostic accuracy of non-invasive 64-slice CT coronary angiography in patients with stable angina pectoris. Eur Radiol 2006; 16: pp. 575-582.
17. Mollet N.R., Cademartiri F., van Mieghem C.A., et. al.: High-resolution spiral computed tomography coronary angiography in patients referred for diagnostic conventional coronary angiography. Circulation 2005; 112: pp. 2318-2323.
18. Ropers D., Rixe J., Anders K., et. al.: Usefulness of multidetector row spiral computed tomography with 64- × 0.6-mm collimation and 330-ms rotation for the noninvasive detection of significant coronary artery stenoses. Am J Cardiol 2006; 97: pp. 343-348.
19. Dewey M., Hoffmann H., Hamm B., et. al.: CT coronary angiography using 16 and 64 simultaneous detector rows: intraindividual comparison. Rofo 2007; 179: pp. 581-586.
20. Lee M.S., Kapoor N., Jamal F., et. al.: Comparison of coronary artery bypass surgery with percutaneous coronary intervention with drug-eluting stents for unprotected left main coronary artery disease. J Am Coll Cardiol 2006; 47: pp. 864-870.
21. Raja S.G.: Drug-eluting stents and the future of coronary artery bypass surgery: facts and fiction. Ann Thorac Surg 2006; 81: pp. 1162-1171.
22. Ong A.T., van der Giessen W.J.: Drug-eluting stents for interventional revascularization of coronary multivessel disease. J Interv Cardiol 2005; 18: pp. 447-453.
23. Breeman A., Hordijk-Trion M., Lenzen M., et. al.: Treatment decisions in stable coronary artery disease: insights from the Euro Heart Survey on Coronary Revascularization. J Thorac Cardiovasc Surg 2006; 132: pp. 1001-1009.
24. Behrenbeck W. Koronarangiographie und perkutane koronarangioplastie. Available from http://www.bqs-qualitaetsreport.de/Webs/bqs/qualrep/2004/ergebnisse/ . Accessed September 2006.
25. Scanlon P.J., Faxon D.P., Audet A.M., et. al.: ACC/AHA guidelines for coronary angiography. J Am Coll Cardiol 1999; 33: pp. 1756-1824.
26. ter Woorst F.J., Berry L.L., de Swart H.J., et. al.: A rare complication of coronary arteriography. Cathet Cardiovasc Diagn 1998; 43: pp. 455-456.
27. Brunner M., Trebing D., Goring H.D.: Cholesterol embolism syndrome after coronary angiography. Hautarzt 2005; 56: pp. 854-859.
28. van Buuren F., Mannebach H., Horstkotte D.: 20th report of performance data from heart catheterization laboratories in Germany. Z Kardiol 2005; 94: pp. 212-215.
29. Devlin G., Lazzam L., Schwartz L.: Mortality related to diagnostic cardiac catheterization. Int J Card Imaging 1997; 13: pp. 379-386.
30. Porzionato A., Zancaner S., Ramondo A., et. al.: Onset and progression of fatal coronary dissection during angiography. Can J Cardiol 2006; 22: pp. 77-78.
31. Dorgelo J., Willems T.P., Geluk C.A., et. al.: Multidetector computed tomography-guided treatment strategy in patients with non-ST elevation acute coronary syndromes: a pilot study. Eur Radiol 2005; 15: pp. 708-713.
32. Hoffmann M.H., Shi H., Schmitz B.L., et. al.: Noninvasive coronary angiography with multislice computed tomography. JAMA 2005; 293: pp. 2471-2478.
33. Kovacs A., Probst C., Sommer T., et. al.: [CT coronary angiography in patients with atrial fibrillation]. Rofo 2005; 177: pp. 1655-1662.
34. Hoffmann M.H., Shi H., Manzke R., et. al.: Noninvasive coronary angiography with 16-detector row CT: effect of heart rate. Radiology 2005; 234: pp. 86-97.
35. Schroeder S., Kuettner A., Beck T., et. al.: Usefulness of noninvasive MSCT coronary angiography as first-line imaging technique in patients with chest pain: initial clinical experience. Int J Cardiol 2005; 102: pp. 469-475.