
Rationale and Objectives
The purpose of the present study was to evaluate the imaging findings of triple-negative breast cancer patients receiving neoadjuvant chemotherapy (NAC) and to investigate whether the findings are different between responders and nonresponders, enabling us to predict the final patient response.
Materials and Methods
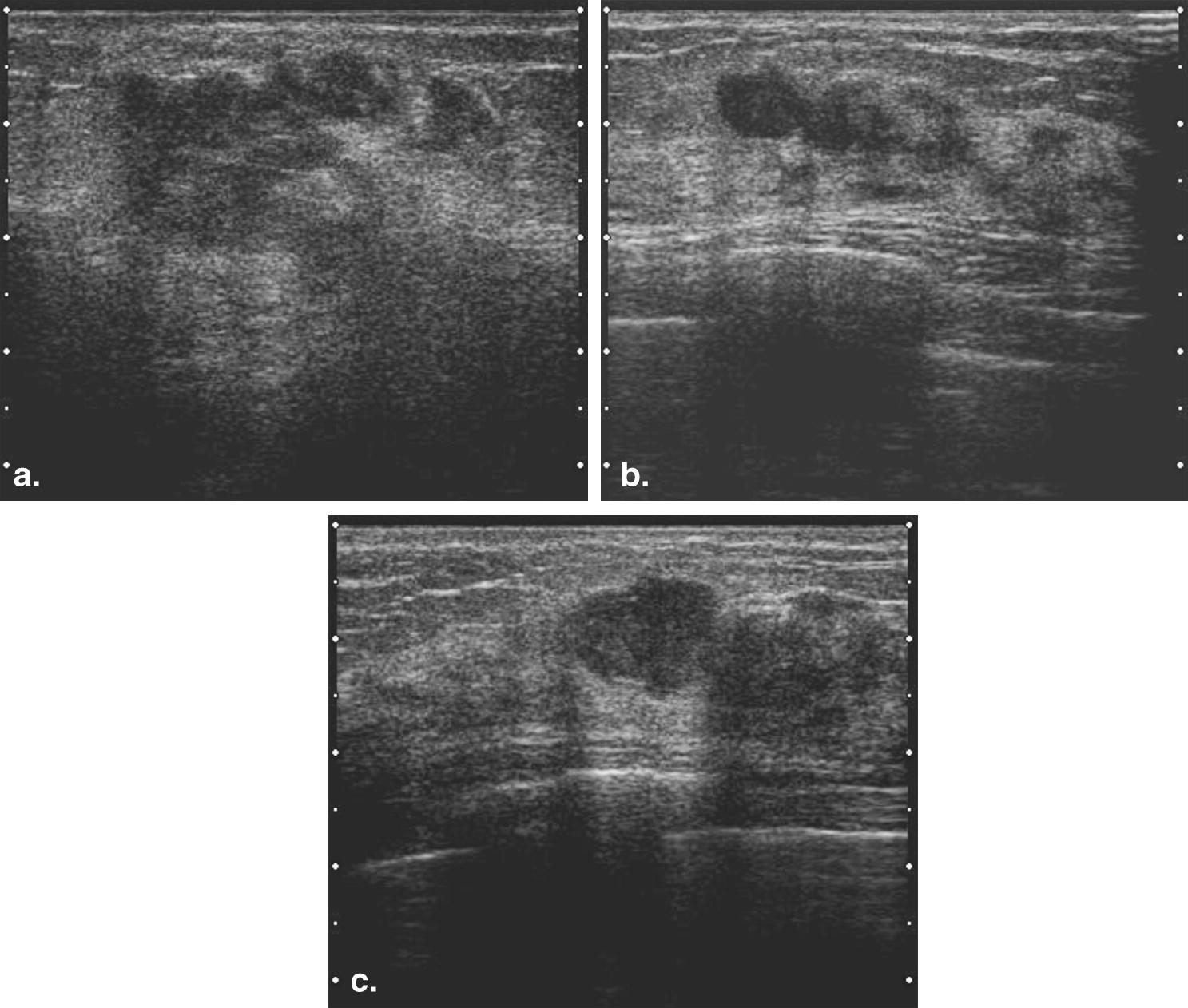
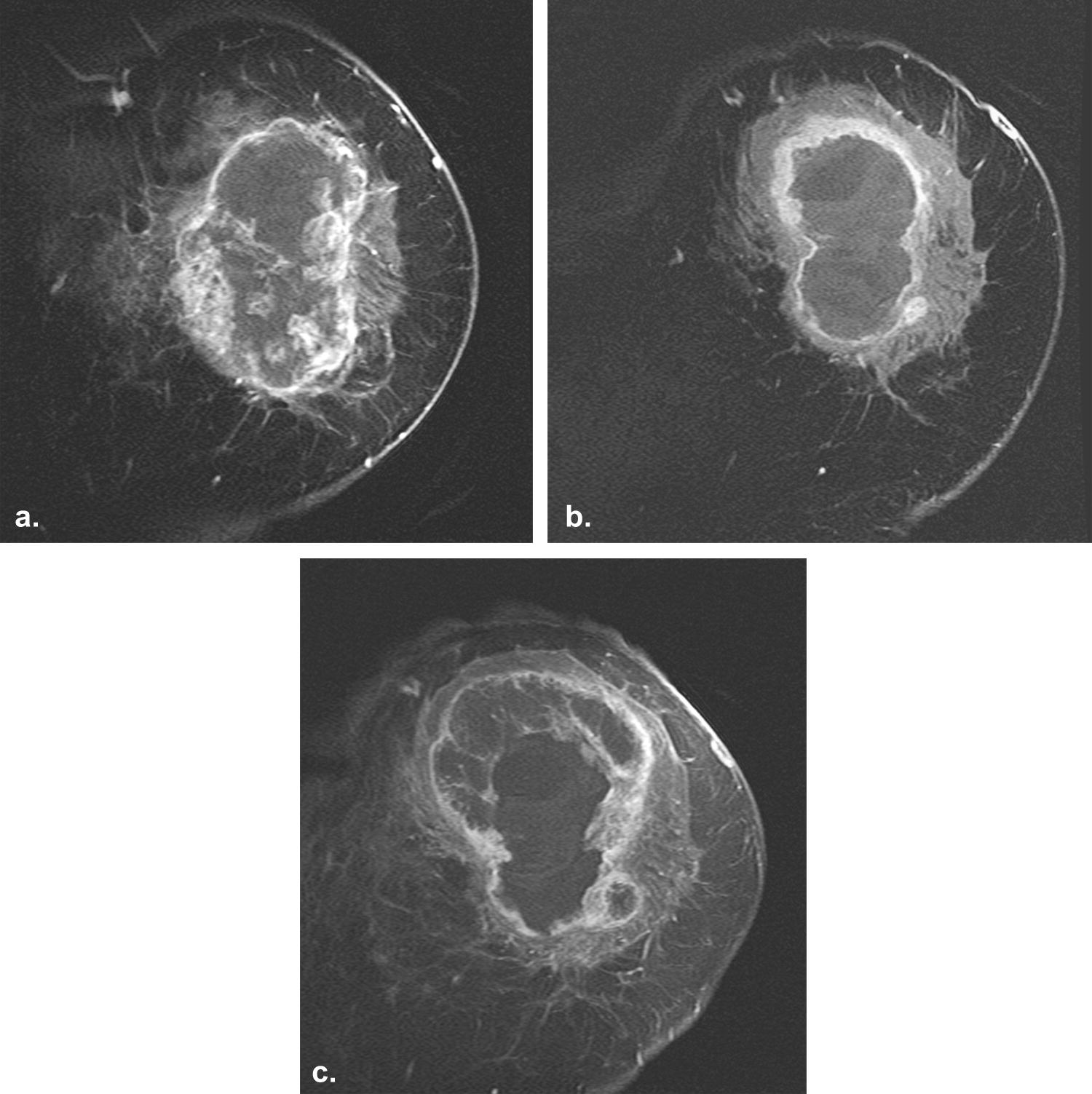
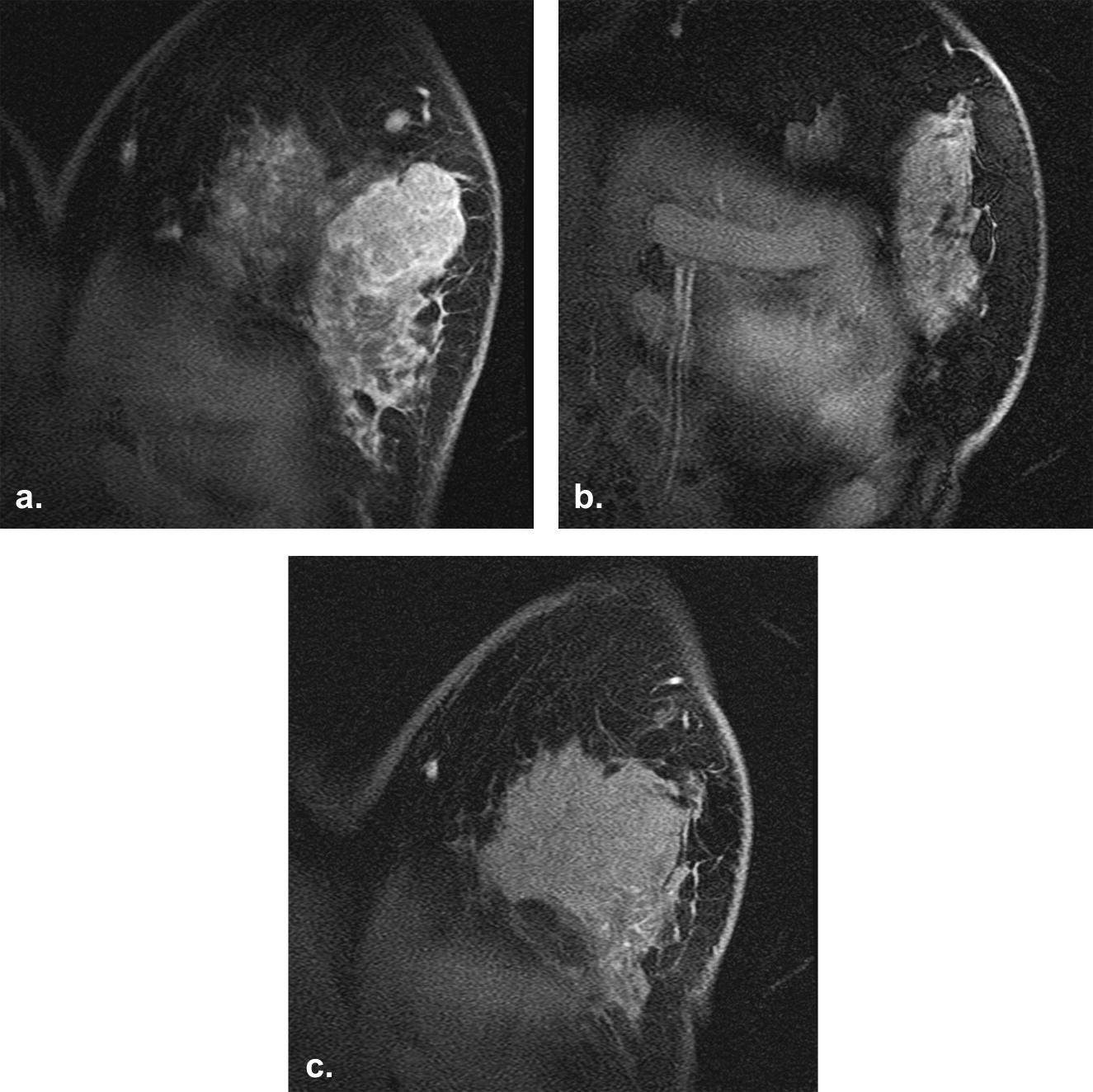
The subjects included 22 women ages 35–73 years (mean, 50.4 years) with 23 triple-negative breast cancers who underwent NAC. In all cases, a mammography, ultrasound, and magnetic resonance imaging (MRI) were performed a total of three times: before NAC, after the first half of NAC, and after NAC. The mass shape, mass margin, presence of clear intratumoral necrosis, and presence of intratumoral calcification were analyzed. The presence of clear intratumoral necrosis was evaluated on the MRI. If there was a very high signal intensity (similar to that of water) in the tumor on the fat-suppressed T2-weighted MRI scans, we judged it to be clear intratumoral necrosis.
Results
An irregularly shaped mass ( P = .018) and the presence of clear intratumoral necrosis ( P = .044) were significantly associated with NAC nonresponse in triple-negative breast cancer patients. The mass margin and the presence of intratumoral calcification were not related to the effects after NAC.
Conclusions
In cases of triple-negative breast cancer involving clear intratumoral necrosis with an irregular mass shape, it is predicted that the effects of neoadjuvant chemotherapy will likely be poor, and therefore, the presence of such image findings may be useful for determining the optimal application of neoadjuvant chemotherapy.
Breast cancer is comparatively sensitive to chemotherapy. In addition, hormone therapy is also effective for hormone receptor–positive breast cancers. Therefore, a multidisciplinary approach, which is directed both to the locoregional control (surgery and radiation therapy) and to the destruction of distant micrometastases (chemotherapy and hormone therapy) has become the main strategy in the treatment of breast cancer. The indication for chemotherapy and hormone therapy is generally decided according to the risk category in the International Consensus Conference on Primary Treatment of Breast Cancer . Triple-negative breast cancers, which are negative for estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor 2 (HER2), are usually resistant tochemotherapy and endocrine therapy, and patients with these tumors have a poor prognosis . However, we are able to clinically identify a triple-negative breast cancer that shows a good response to chemotherapy.
Neoadjuvant chemotherapy (NAC) has been the standard treatment for locally advanced breast cancer. NAC is mainly designed to reduce tumor size, thereby permitting breast-conserving surgery . Other advantages for NAC are that systemic therapy may be initiated earlier and enables the evaluation of a patient’s response to chemotherapy . Conversely, a NAC-related disadvantage is the delay in surgical treatment in patients who do not respond to chemotherapy. If we can predict the final chemotherapeutic response during earlier courses of NAC, an earlier and optimized treatment regimen is possible, thereby improving the patient prognosis .
Get Radiology Tree app to read full this article<
Materials and methods
Patients and Treatment
Get Radiology Tree app to read full this article<
Table 1
Patient Population
No Age TNM Histological Type Chemotherapy Maximum Diameter (mm) Before NAC (MRI) Maximum Diameter (mm) After NAC (Pathology) Overall Response to NAC 1 56 T4aN1M0 IDC EC4DOC2EC2 75 75 SD 2 50 T2N0M1 IDC FEC6 25 18 SD 3 44 T2N0M0 IDC FEC4DOC4 26 (-) CR 4 44 T1bN0M0 IDC FEC4DOC4 6 1 Near CR 5 36 T2N0M0 IDC FEC4DOC4 40 (-) CR 6 60 T2N0M0 IDC FEC4DOC4 40 DCIS only Near CR 7 52 T3N1M0 IDC FEC4DOC4 60 22 PD (new lesion) 8 43 T4cN3cM0 IDC FEC4 100 110 SD 9 44 T2N0M0 Pleomorphic carcinoma FEC4DOC4 40 32 SD 10 55 T2N0M0 IDC FEC4DOC4 38 35 SD 11 61 T2N1M0 IDC FEC4DOC4 26 (-) CR 12 35 T1cN1M0 IDC FEC4DOC4 18 15 SD 13 41 T3N3bM0 IDC FEC4DOC2 85 110 ∗ (MRI) PD 14 45 T2N1M0 IDC FEC4DOC4 25 40 PD 15 61 T2N1M0 IDC FEC4DOC4 25 9 PR 16 73 T4dN1M0 IDC FEC4DOC4 50 41 SD 17 42 T2N0M0 IDC FEC4DOC4 22 (-) CR 18 54 T2N0M0 IDC FEC4DOC4 34 20 PR 19 50 T2N0M0 IDC FEC4DOC4 22 5 PR 20 47 T2N0M0 IDC FEC4DOC2 35 18 SD (regrowth) 21 65 T2N0M0 IDC FEC4DOC4 21 2 near CR 22 48 T2N0M0 IDC FEC4DOC4 21 2 near CR 23 54 T2N0M0 IDC FEC4DOC4 22 4 PR
(-), pathological complete response; DCIS, ductal carcinoma in situ; IDC, invasive ductal carcinoma; NAC, neoadjuvant chemotherapy.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Imaging Methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Image Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Histopathology
Get Radiology Tree app to read full this article<
Therapeutic Response Evaluation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Comparison of Imaging Findings Between Good Responders and Nonresponders
Imaging Finding Good Responders ( n = 8) Nonresponders ( n = 11)P Value Mass shape Round, oval, lobulated 8 5 .018 Irregular 0 6 Mass margin Smooth 5 5 NS Irregular 3 6 Clear intratumoral necrosis Presence 0 5 .044 Absence 8 6 Intratumoral calcification on mammogram Presence 2 3 NS Absence 6 8
NS, not significant.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Goldhirsch A., Ingle J.N., Gelber R.D., et. al.: Thresholds for therapies: highlights of the St Gallen international expert consensus on the primary therapy of early breast cancer 2009. Ann Oncol 2009; 20: pp. 1319-1329.
2. Bauer K.R., Brown M., Cress R.D., et. al.: Descriptive analysis of estrogen receptor (ER)-negative, progesterone receptor (PR)-negative, and HER2-negative invasive breast cancer, the so-called triple-negative phenotype. Cancer 2007; 109: pp. 1721-1728.
3. Rakha E.A., Reis-Filho J.S., Ellis I.O.: Basal-like breast cancer: a critical review. J Clin Oncol 2008; 26: pp. 2568-2581.
4. Cheang M.G., Voduc D., Bajdik C., et. al.: Basal-like breast cancer defined by five biomarkers has superior prognostic value than triple-negative phenotype. Clin Cancer Res 2008; 14: pp. 1368-1376.
5. Haffty B.G., Yang Q., Reiss M., et. al.: Locoregional relapse and distant metastasis in conservatively managed triple negative early-stage breast cancer. J Clin Oncol 2006; 24: pp. 5652-5657.
6. Mersin H., Yildirim E., Berberoglu U., et. al.: The prognostic importance of triple negative breast carcinoma. Breast 2008; 17: pp. 341-346.
7. Wolmark N., Wang J., Mamounas E., et. al.: Preoperative chemotherapy in patients with operable breast cancer: nine-year results from National Surgical Adjuvant Breast and Bowel Project B-18. J Natl Cancer Inst Monogr 2001; 30: pp. 96-102.
8. Smith I.C., Heys S.D., Hutcheon A.W., et. al.: Neoadjuvant chemotherapy in breast cancer: significantly enhanced response with docetaxel. J Clin Oncol 2002; 20: pp. 1456-1466.
9. Kaufmann M., Hortobagyi G.N., Goldhirsch A., et. al.: Recommendations from an international expert panel on the use of neoadjuvant primary systemic treatment of operable breast cancer: an update. J Clin Oncol 2006; 24: pp. 1940-1949.
10. Therasse P., Arbuck S.G., Eisenhauer E.A., et. al.: New guidelines to evaluate the response to treatment in solid tumors. JNCI 2000; 92: pp. 205-216.
11. Abraham D.C., Jones R.C., Jones S.E., et. al.: Evaluation of neoadjuvant chemotherapeutic response of locally advanced breast cancer by magnetic resonance imaging. Cancer 1996; 78: pp. 91-100.
12. Balu-Maestro C., Chapellier C., Bleuse A., et. al.: Imaging in evaluation of response to neoadjuvant breast cancer treatment: benefits of MRI. Breast Cancer Res Treat 2002; 72: pp. 145-152.
13. Weatherall P.T., Evans G.F., Metzger G.J., et. al.: MRI vs. histologic measurement of breast cancer following chemotherapy: comparison with x-ray mammography and palpation. J Magn Reson Imaging 2001; 13: pp. 868-875.
14. Londero V., Bazzocchi M., Frate C.D., et. al.: Locally advanced breast cancer: comparison of mammography, sonography and MR imaging in evaluation of residual disease in women receiving neoadjuvant chemotherapy. Eur Radiol 2004; 14: pp. 1371-1379.
15. Chen J.H., Feig B., Agrawal G., et. al.: MRI evaluation of pathologically complete response and residual tumors in breast cancer after neoadjuvant chemotherapy. Cancer 2008; 112: pp. 17-26.
16. Cheung Y.C., Chen S.C., Su M.Y., et. al.: Monitoring the size and response of locally advanced breast cancers to neoadjuvant chemotherapy (weekly paclitaxel and epirubicin) with serial enhanced MRI. Breast Cancer Res Treat 2003; 78: pp. 51-58.
17. Rieber A., Zeitler H., Rosenthal H., et. al.: MRI of breast cancer: influence of chemotherapy on sensitivity. Br J Radiol 1997; 70: pp. 452-458.
18. Rieber A., Brambs H.J., Gabelmann A., et. al.: Breast MRI for monitoring response of primary breast cancer to neo-adjuvant chemotherapy. Eur Radiol 2002; 12: pp. 1711-1719.
19. Ah-See M.L., Makris A., Taylor N.J., et. al.: Early changes in functional dynamic magnetic resonance imaging predict for pathologic response to neoadjuvant chemotherapy in primary breast cancer. Clin Cancer Res 2008; 14: pp. 6580-6589.
20. Khoury C.E., Servois V., Thibault F., et. al.: MR quantification of the washout changes in breast tumors under preoperative chemotherapy: feasibility and preliminary results. Am J Roentgenol 2005; 184: pp. 1499-1504.
21. Chou C.P., Wu M.T., Chang H.T., et. al.: Monitoring breast cancer response to neoadjuvant systemic chemotherapy using parametric contrast-enhanced MRI: a pilot study. Acad Radiol 2007; 14: pp. 561-573.
22. Uematsu T., Kasami M., Yuen S.: Triple-negative breast cancer: correlation between MR imaging and pathologic findings. Radiology 2009; 250: pp. 638-647.
23. Fisher E.R., Anderson S., Redmond C., et. al.: Pathologic findings from the National Surgical Adjuvant Breast Project B-06: 10-year pathologic and clinical prognostic discriminants. Cancer 1993; 71: pp. 2507-2514.
24. Jimenez R.E., Wallis T., Visscher D.W.: Centrally necrotizing carcinoma of the breast: a distinct histologic subtype with aggressive clinical behavior. Am J Surg Pathol 2001; 25: pp. 331-337.
25. Leek R.D., Landers R.J., Harris A.L., et. al.: Necrosis correlates with high vascular density and focal macrophage infiltration in invasive carcinoma of the breast. Br J Cancer 1999; 79: pp. 991-995.
26. Metz S., Daldrup-Link H.E., Richter T., et. al.: Detection and quantification of breast tumor necrosis with MR imaging: value of the necrosis-avid contrast agent Gadophrin-3. Acad Radiol 2003; 10: pp. 484-490.