
Rationale and Objective
The aim of this study was to compare image quality on dedicated and triple rule-out coronary computed tomographic (CT) angiography (CTA) with respect to motion artifacts and the quality of coronary artery opacification.
Materials and Methods
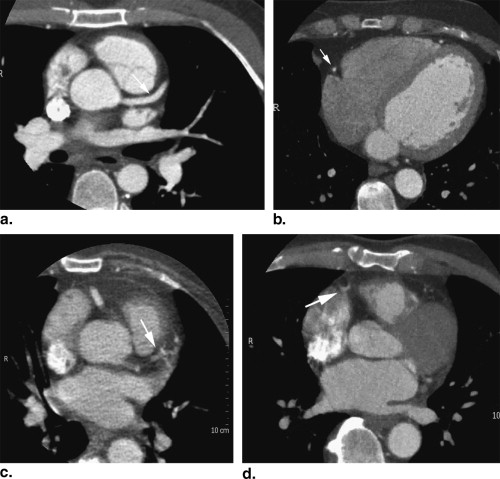
Twenty dedicated coronary CT angiographic studies and 20 emergency department triple rule-out CT angiographic studies (ie, to rule out pulmonary embolism, aortic dissection, and acute coronary syndrome) performed on 64-slice CT scanner were selected. Two radiologists, blinded to type of CTA, scored coronary artery image quality. Up to 14 coronary artery segments were scored for motion artifact on a scale ranging from 1 (no motion artifact) to 4 (severe motion artifact). The radiologists also scored the quality of opacification (1 = good opacification, 2 = limited opacification, 3 = vessel not seen). The average of all segments and dedicated larger and smaller coronary artery segments was compared.
Results
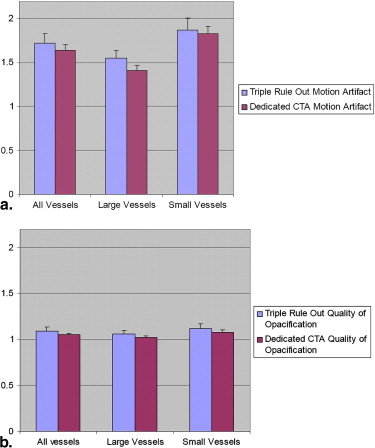
The average motion-artifact scores per vessel segment for dedicated and triple rule-out studies were 1.64 and 1.72, respectively ( P = .6). For larger segments, the average motion-artifact score was 1.41 for dedicated CTA compared to 1.55 for triple rule-out CTA ( P = .2). The average coronary artery opacification for dedicated studies was 1.05 for all segments and 1.03 for larger segments, compared to triple rule-out studies, which had scores of 1.09 ( P = .5) for all segments and 1.06 ( P = .5) for larger segments. No statistically significant differences in favor of dedicated CTA were identified.
Conclusion
The image quality of triple rule-out CTA is comparable to that of dedicated coronary CTA, showing no statistically significant difference in motion artifacts or opacification, and therefore may be an alternative and useful diagnostic study in a select group of emergency department patients.
Since the development of multidetector computed tomography more than a decade ago, coronary artery computed tomographic (CT) angiography (CTA) has become much more widespread. Current 64-slice multidetector computed tomography, with higher spatial and temporal resolution and better longitudinal coverage, permits improved and more consistent visualization of the coronary arteries .
Coronary artery evaluation using CTA has traditionally been performed in an outpatient setting in patients with atypical chest pain with risk factors for coronary artery disease. Patients with equivocal stress test results may also be referred for coronary CTA . Dedicated coronary CT imaging is performed with electrocardiographic gating and a small field of view restricted to the heart, to optimize spatial resolution for the evaluation of the coronary arteries .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Patients
Get Radiology Tree app to read full this article<
Table 1
Patient Demographic Information
Study Number of Patients Age Range (y) Average Age (y) Average (range) Heart Rate (beats/min) Men/Women Triple rule-out CTA 20 26–61 49 66 (40–84) 11/9 Dedicated CTA 20 33–69 49 64 (54–77) 13/7
CTA, computed tomographic angiography.
Get Radiology Tree app to read full this article<
CT Protocols and Acquisition
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Scan Acquisition Parameters for Retrospective Electrocardiographically Gated (without tube current modulation) Dedicated Coronary Artery CTA and Triple Rule-Out CTA with Respective Radiation Dose Values
Parameter Routine Chest CT Pulmonary Embolism Chest CT Dedicated Coronary Artery CTA Triple Rule-Out CTA IV contrast (mL) 100 100 100 130 Scan direction Craniocaudal Caudocranial Craniocaudal Caudocranial Scan length (cm) 31 29 17 30 Field of view 400 400 220 400 Rotation time (s) 0.5 0.5 0.4 0.4 Pitch 1.08 0.67 0.2 0.2 Tube voltage (kVp) 120 120 120 120 Current-time product (mAs) 200 370 800 850 CTDI (mGy) 10.6 18 47 50 DLP ∗ (mGy × cm) 376.7 594.3 1242.7 1891.4 Effective dose † (mSv) 6.4 10.1 21.1 32.2
CT, computed tomography; CTA, computed tomographic angiography; CTDI, computed tomographic dose index; DLP, dose-length product; IV, intravenous.
Non–electrocardiographically gated routine chest and pulmonary embolism computed tomographic protocols are also included for reference.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CT Analysis
Get Radiology Tree app to read full this article<
Table 3
Sample Score Sheet
Patient #1 Motion Artifact (1 = no motion; 2 = minimal; 3 = moderate; 4 = severe, vessel cannot be assessed) Quality of Opacification (1 = good, 2 = limited opacification, 3 = not seen) Left main ∗ 1 2 3 4 1 2 3 Proximal LAD ∗ 1 2 3 4 1 2 3 Mid LAD ∗ 1 2 3 4 1 2 3 Proximal circumflex ∗ 1 2 3 4 1 2 3 Proximal RCA ∗ 1 2 3 4 1 2 3 Mid RCA ∗ 1 2 3 4 1 2 3 Distal LAD 1 2 3 4 1 2 3 First diagonal 1 2 3 4 1 2 3 Distal RCA 1 2 3 4 1 2 3 Distal circumflex 1 2 3 4 1 2 3 PDA 1 2 3 4 1 2 3 Posterolateral 1 2 3 4 1 2 3 Obtuse marginal 1 2 3 4 1 2 3 Ramus 1 2 3 4 1 2 3
LAD, left anterior descending; PDA, posterior descending artery; RCA, right coronary artery.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Table 4
Advantages and Disadvantages of Dedicated Coronary CTA and the Triple Rule-out CTA
Triple Rule-out CTA Dedicated Coronary Artery CTA Advantages (1) Evaluates cardiac and extracardiac etiologies of chest pain, including the aorta and pulmonary arteries (1) Lower radiation dose than triple rule-out protocol; (2) lower IV contrast volume Disadvantages (1) Higher radiation dose than dedicated coronary artery CTA; (2) larger IV contrast volume; (3) longer breath hold (1) Provides limited evaluation of aorta and pulmonary arteries; (2) high radiation dose
CTA, computed tomographic angiography; IV, intravenous.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Acknowledgment
Get Radiology Tree app to read full this article<
References
1. Pannu H.K., Jacobs J.E., Lai S., et. al.: Coronary CT Angiography with 64-MDCT: assessment of vessel visibility. AJR Am J Roentgenol 2006; 187: pp. 119-126.
2. Schoepf U.J., Zwerner P.L., Savino G., Herzog C., Kerl J.M., Costello P.: Coronary CT angiography. Radiology 2007; 244: pp. 48-63.
3. Nicolau K., Knez A., Rist C., et. al.: Accuracy of 64-MDCT in the diagnosis of ischemic heart disease. AJR Am J Roentgenol 2006; 187: pp. 111-117.
4. Hoffman U., Nagurney J.T., Moselewski F., et. al.: Coronary multidetector computed tomography in the assessment of patients with acute chest pain. Circulation 2006; 114: pp. 2251-2260.
5. McCraig L.F., Burt C.S.: National Hospital Ambulatory Medical Care Survey: 2003 emergency department summary. Advocate data from vital and health statistics; no 358.2005.National Center for Health StatisticsHyattsville, MD
6. Tosteson A.N., Goldman L., Udvarhelyi I.S., et. al.: Cost-effectiveness of a coronary care unit versus an intermediate care unit for emergency department patients with chest pain. Circulation 1996; 94: pp. 143-150.
7. Storrow A.B., Gibler W.B.: Chest pain centers: diagnosis of acute coronary syndromes. Ann Emerg Med 2000; 35: pp. 449-461.
8. Takakuwa K.M., Halpern E.J.: Evaluation of a “triple rule-out” coronary CT angiography protocol: use of 64-section CT in low-to-moderate risk emergency department patients suspected of having acute coronary syndrome. Radiology 2008; 248: pp. 438-446.
9. White C.S., Kuo D.: Chest pain in the emergency department: role of multidetector CT. Radiology 2007; 245: pp. 672-681.
10. White C.S., Kuo D., Kelemen M., et. al.: Chest pain evaluation in the emergency room: can multi-slice CT provide a comprehensive evaluation?. AJR Am J Roentgenol 2005; 185: pp. 533-540.
11. Budoff M.J., Achenbach S., Blumenthal R.S., et. al.: Assessment of coronary artery disease by cardiac computed tomography: a scientific statement from the American Heart Association Committee on Cardiovascular Imaging and Intervention, and Committee on Cardiac Imaging, Council on Clinical Cardiology. Circulation 2006; 114: pp. 1761-1791.
12. Budoff M.J.: Cardiac CT in the emergency room. Appl Radiol 2006; 35: pp. 48-55.
13. Flukinger T., White C.S.: Multidetector computed tomography in the evaluation of chest pain in the emergency department. Semin Roentgenol 2008; 43: pp. 136-144.