
Rationale and Objectives
The aim of this study was to prospectively investigate the diagnostic value of triple rule-out computed tomography (CT) in patients suspected of having acute pulmonary embolism (PE).
Materials and Methods
A total of 125 patients with suspicion of PE, of whom 14 patients had the additional clinical suspicion of acute aortic syndrome, underwent electrocardiogram-gated triple rule-out dual-source CT. The contrast media application protocol was adjusted to obtain a homogenous attenuation of the pulmonary arteries, thoracic aorta, and coronary arteries. The diagnostic performance of triple rule-out CT was assessed by using adjudicated discharge diagnoses as reference standards.
Results
A total of 161 adjudicated cardiovascular discharge diagnoses were made in the 125 patients (including all true-positive and true-negative findings): acute PE was found in 26 (21%) and was excluded by CT in 99 (79%), coronary artery disease was found in 3 (3%) and was excluded by catheter angiography in 9 (6%), left ventricular systolic dysfunction was found in 2 (2%) and was excluded by echocardiography in 8 (6%), and acute aortic syndrome was found in 5 (4%) and was excluded by CT in 9 (7%) patients. Nonvascular chest disease was found in 34 (27%) and included pneumonia ( n = 17), neoplasms (n = 5), fractures/osteolysis ( n = 3), pericarditis ( n = 2), and post-pneumonectomy syndrome ( n = 1). Triple rule-out CT was normal in 53 (42%) patients. Overall sensitivity, specificity, and positive and negative predictive value of triple rule-out CT for cardiovascular disease were 100% (95% confidence interval [CI] 90–100%), 98% (95%CI 94–100%), 95% (95%CI 82–99%), and 100% (95%CI 97–100%, respectively).
Conclusions
Triple rule-out CT is feasible in patients with suspicion of PE, reveals a wide range of vascular and non-vascular chest disease, and offers an excellent overall diagnostic performance.
The diagnosis of pulmonary embolism (PE) remains a challenge because clinical signs and symptoms of PE are nonspecific . Various pathologies such as pneumonia, pneumothorax, pericarditis as well as more life-threatening conditions such as acute coronary syndrome (ACS) or acute aortic syndrome (AAS) may present with similar complaints, and an overlap between these diseases exists . Thus, a significant number of emergency department patients often receive simultanous testing for at least two of these diseases .
The probability of having PE is estimated based on the risk factors for thromboembolic events combined with the signs and symptoms of the patient. However, the estimation may be insufficient to rule out or to diagnose the disease with certainty. Thus, an imaging examination is often required to achieve a definite diagnosis . Currently, multidetector computed tomography (CT) with a non-electrocardiography (ECG)-gated, contrast-enhanced pulmonary angiogram represents the standard imaging modality when PE is suspected . However, pathologies involving the coronary arteries and aortic root, such as ACS and AAS, cannot be sufficently evaluated with a non–ECG-gated CT protocol because of cardiac motion artifacts.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Patient Population
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
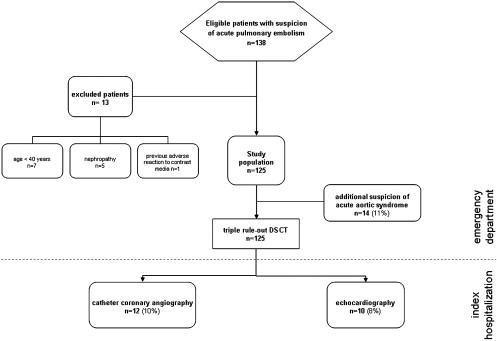
Table 1
Patient Characteristics
Patients Total 125 Age, y 59.3 ± 15.2 Men (%) 58 (46.4) Body mass index 27.3 ± 6.3 (15.3–47) Symptoms Chest pain (%) 49 (39.2) Dyspnea (%) 35 (28) Hypoxemia (%) 6 (4.8) Tachypnoea (%) 6 (4.8) Syncope (%) 5 (4) Cough (%) 5 (4) Hemoptysis (%) 1 (0.8) Comorbidity and cardiovascular risk factors Cancer (%) 31 (24.8) Surgery within 2 months (%) 11 (8.8) Trauma within 2 months (%) 3 (2.4) Prior pulmonary embolism (%) 7 (5.6) Deep vein thrombosis (%) 4 (3.2) Urosepsis (%) 1 (0.8) Pancreatitis (%) 1 (0.8) Chronic obstructive lung disease (%) 7 (5.6) Hypertension (%) 46 (36.8) Hyperlipidemia (%) 20 (16) Nicotine (%) 27 (21.6)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Triple Rule-out CT
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Data Analysis
Image Quality
Get Radiology Tree app to read full this article<
Chest Disease
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Reference Standards
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Image Quality
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Vascular Pathology
Acute PE
Get Radiology Tree app to read full this article<

Table 2
Triple Rule-out Dual-source CT Findings in Patients Suspected to have Pulmonary Embolism
Dual-source CT findings Number of patients ( n = 125) No chest pathology (%) 53 (42) Vascular pathologies of the chest, total (%) 38 (30.4) Acute pulmonary embolism, total (%) 26 (21) Central (%) 1 (1) Paracentral (%) 1 (1) Lobar (%) 0 (0) Segmental (%) 10 (8) Subsegmental (%) 7 (6) Paracentral and segmental (%) 2 (2) Segmental and subsegmental (%) 5 (4) Acute aortic syndrome, total (%) 5 (4) Type A dissection (%) 1 (1) Type B dissection (%) 3 (2) Plaque rupture (%) 1 (1) Coronary artery disease, total ∗ (%) 4 (3) Significant stenosis of the RCA (%) 3 ∗∗ Significant stenosis of the LAD (%) 4 ∗∗∗ Acute coronary syndrome 0 Left ventricular systolic dysfunction (%) 3 (2) Nonvascular pathologies of the chest, total (%) 34 (27) Pneumonia/consolidation (%) 17 (14) Postpneumonectomy syndrome (%) 1 (1) Pericarditis (%) 2 (2) Neoplasm (%) 5 (4) Skeletal (%) 3 (2) Osteolytic bone lesion (%) 1 (1) Acute fracture of a rib (%) 1 (1) Acute fracture of L1 (%) 1 (1)
CT, computed tomography; RCA, right coronary artery; LAD, left anterior descending artery.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
AAS
Get Radiology Tree app to read full this article<
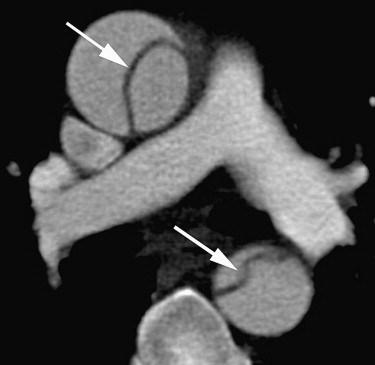
Get Radiology Tree app to read full this article<
CAD
Get Radiology Tree app to read full this article<
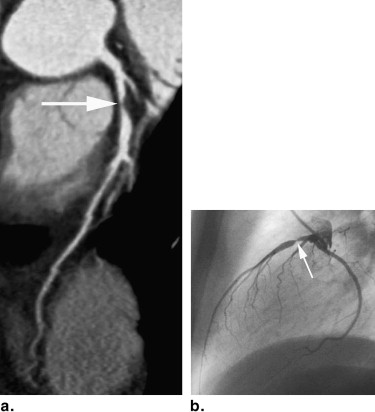
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
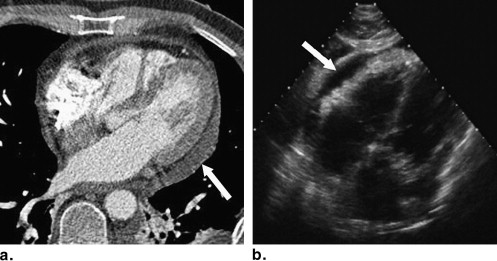
LV Systolic Dysfunction
Get Radiology Tree app to read full this article<
Diagnostic Performance of Triple Rule-out CT
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Diagnostic Performance of Triple Rule-out Dual-source CT for Diagnosing Cardiovascular Disease ∗ in Patients Suspected to have Pulmonary Embolism
n TP TN FP FN Sensitivity Specificity PPV NPV Accuracy Triple rule-out CT 161 36 123 2 0 100% (90–100%) 98% (94–100%) 95% (82–99%) 100% (97–100%) 99% (96–100%)
TP, true positive; TN, true negative; FP, false positive; FN, false negative; PPV, positive predictive value; NPV, negative predictive value.
Values in parenthesis are 95% confidence intervals.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Nonvascular Pathology
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
PE
Get Radiology Tree app to read full this article<
AAS
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
CAD
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
LV Systolic Dysfunction
Get Radiology Tree app to read full this article<
Radiation Dose
Get Radiology Tree app to read full this article<
Study Limitations
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Goldhaber S.Z.: Pulmonary embolism. Lancet 2004; 363: pp. 1295-1305.
2. Rogg J.G., Neve J.W., Huang C., et. al.: The triple work-up for emergency department patients with acute chest pain: how often does it occur?. J Emerg Med 2008; Sep 12 [Epub ahead of print]
3. Chunilal S.D., Eikelboom J.W., Attia J., et. al.: Does this patient have pulmonary embolism?. JAMA 2003; 290: pp. 2849-2858.
4. Remy-Jardin M., Pistolesi M., Goodman L.R., et. al.: Management of suspected acute pulmonary embolism in the era of CT angiography: a statement from the Fleischner Society. Radiology 2007; 245: pp. 315-329.
5. Schoepf U.J., Costello P.: CT angiography for diagnosis of pulmonary embolism: state of the art. Radiology 2004; 230: pp. 329-337.
6. Schoepf U.J., Goldhaber S.Z., Costello P.: Spiral computed tomography for acute pulmonary embolism. Circulation 2004; 109: pp. 2160-2167.
7. Flohr T.G., McCollough C.H., Bruder H., et. al.: First performance evaluation of a dual-source CT (DSCT) system. Eur Radiol 2006; 16: pp. 256-268.
8. Achenbach S., Ropers D., Kuettner A., et. al.: Contrast-enhanced coronary artery visualization by dual-source computed tomography–initial experience. Eur J Radiol 2006; 57: pp. 331-335.
9. Matt D., Scheffel H., Leschka S., et. al.: Dual-source CT coronary angiography: image quality, mean heart rate, and heart rate variability. AJR Am J Roentgenol 2007; 189: pp. 567-573.
10. Johnson T.R., Nikolaou K., Wintersperger B.J., et. al.: Dual-source CT cardiac imaging: initial experience. Eur Radiol 2006; 16: pp. 1409-1415.
11. Schertler T., Scheffel H., Frauenfelder T., et. al.: Dual-source computed tomography in patients with acute chest pain: feasibility and image quality. Eur Radiol 2007; 17: pp. 3179-3188.
12. Johnson T.R., Nikolaou K., Becker A., et. al.: Dual-source CT for chest pain assessment. Eur Radiol 2008; 18: pp. 773-780.
13. Yamamuro M., Tadamura E., Kubo S., et. al.: Cardiac functional analysis with multi-detector row CT and segmental reconstruction algorithm: comparison with echocardiography, SPECT, and MR imaging. Radiology 2005; 234: pp. 381-390.
14. Dogan H., Kroft L.J., Huisman M.V., et. al.: Right ventricular function in patients with acute pulmonary embolism: analysis with electrocardiography-synchronized multi-detector row CT. Radiology 2007; 242: pp. 78-84.
15. Takakuwa K.M., Halpern E.J.: Evaluation of a “triple rule-out” coronary CT angiography protocol: use of 64-Section CT in low-to-moderate risk emergency department patients suspected of having acute coronary syndrome. Radiology 2008; 248: pp. 438-446.
16. Stillman A.E., Oudkerk M., Ackerman M., et. al.: Use of multidetector computed tomography for the assessment of acute chest pain: a consensus statement of the North American Society of Cardiac Imaging and the European Society of Cardiac Radiology. Eur Radiol 2007; 17: pp. 2196-2207.
17. Wells P.S., Anderson D.R., Rodger M., et. al.: Derivation of a simple clinical model to categorize patients probability of pulmonary embolism: increasing the models utility with the SimpliRED D-dimer. Thromb Haemost 2000; 83: pp. 416-420.
18. Leschka S., Scheffel H., Desbiolles L., et. al.: Image quality and reconstruction intervals of dual-source CT coronary angiography: recommendations for ECG-pulsing windowing. Invest Radiol 2007; 42: pp. 543-549.
19. Stolzmann P., Scheffel H., Schertler T., et. al.: Radiation dose estimates in dual-source computed tomography coronary angiography. Eur Radiol 2008; 18: pp. 592-599.
20. Hausleiter J., Meyer T., Hadamitzky M., et. al.: Radiation dose estimates from cardiac multislice computed tomography in daily practice: impact of different scanning protocols on effective dose estimates. Circulation 2006; 113: pp. 1305-1310.
21. Salem R., Remy-Jardin M., Delhaye D., et. al.: Integrated cardio-thoracic imaging with ECG-Gated 64-slice multidetector-row CT: initial findings in 133 patients. Eur Radiol 2006; 16: pp. 1973-1981.
22. Wittram C., Waltman A.C., Shepard J.A., Halpern E., Goodman L.R.: Discordance between CT and angiography in the PIOPED II study. Radiology 2007; 244: pp. 883-889.
23. Quiroz R., Kucher N., Zou K.H., et. al.: Clinical validity of a negative computed tomography scan in patients with suspected pulmonary embolism: a systematic review. JAMA 2005; 293: pp. 2012-2017.
24. Weber T., Auer J., Eber B., et. al.: Value of d-dimer testing in acute aortic dissection. Circulation 2004; 109: pp. E24.
25. Hayter R.G., Rhea J.T., Small A., et. al.: Suspected aortic dissection and other aortic disorders: multi-detector row CT in 373 cases in the emergency setting. Radiology 2006; 238: pp. 841-852.
26. Roos J.E., Willmann J.K., Weishaupt D., et. al.: Thoracic aorta: motion artifact reduction with retrospective and prospective electrocardiography-assisted multi-detector row CT. Radiology 2002; 222: pp. 271-277.
27. White C., Read K., Kuo D.: Assessment of chest pain in the emergency room: what is the role of multidetector CT?. Eur J Radiol 2006; 57: pp. 368-372.
28. Hoffmann U., Nagurney J.T., Moselewski F., et. al.: Coronary multidetector computed tomography in the assessment of patients with acute chest pain. Circulation 2006; 114: pp. 2251-2260.
29. Hoffmann U., Pena A.J., Moselewski F., et. al.: MDCT in early triage of patients with acute chest pain. AJR Am J Roentgenol 2006; 187: pp. 1240-1247.
30. Rubinshtein R., Halon D.A., Gaspar T., et. al.: Usefulness of 64-slice multidetector computed tomography in diagnostic triage of patients with chest pain and negative or nondiagnostic exercise treadmill test result. Am J Cardiol 2007; 99: pp. 925-929.
31. Gallagher M.J., Ross M.A., Raff G.L., et. al.: The diagnostic accuracy of 64-slice computed tomography coronary angiography compared with stress nuclear imaging in emergency department low-risk chest pain patients. Ann Emerg Med 2007; 49: pp. 125-136.
32. Goldstein J.A., Gallagher M.J., O’Neill W.W., et. al.: A randomized controlled trial of multi-slice coronary computed tomography for evaluation of acute chest pain. J Am Coll Cardiol 2007; 49: pp. 863-871.
33. Mollet N.R., Cademartiri F., van Mieghem C.A., et. al.: High-resolution spiral computed tomography coronary angiography in patients referred for diagnostic conventional coronary angiography. Circulation 2005; 112: pp. 2318-2323.
34. Gerber T.C., Kuzo R.S., Morin R.L.: Techniques and parameters for estimating radiation exposure and dose in cardiac computed tomography. Int J Cardiovasc Imaging 2005; 21: pp. 165-176.
35. Einstein A.J., Moser K.W., Thompson R.C., et. al.: Radiation dose to patients from cardiac diagnostic imaging. Circulation 2007; 116: pp. 1290-1305.
36. Ioannidis J.P., Salem D., Chew P.W., et. al.: Accuracy of imaging technologies in the diagnosis of acute cardiac ischemia in the emergency department: a meta-analysis. Ann Emerg Med 2001; 37: pp. 471-477.
37. Raff G.L., Gallagher M.J., O’Neill W.W., et. al.: Diagnostic accuracy of noninvasive coronary angiography using 64-slice spiral computed tomography. J Am Coll Cardiol 2005; 46: pp. 552-557.