
Rationale and Objectives
The aim of our study was to evaluate changes in growth kinetics of breast cancer liver metastasis in response to locoregional therapy and compare them to Response Evaluation Criteria in Solid Tumors (RECIST).
Materials and Methods
This Health Insurance Portability and Accountability Act–compliant retrospective study was Institutional Review Board approved. Thirty-four chemorefractory breast cancer liver metastases from 21 patients treated with yttrium-90 ( 90 Y) were evaluated. Pre- and posttreatment computed tomography (CT) scans were used to calculate tumor growth kinetics. The growth parameter analyzed was reciprocal of doubling time (RDT). RDT range for stable disease (SD) was defined by the measurement error rate. A negative RDT below the SD range defined response and was categorized as either partial response (PR) or complete response, whereas a positive RDT value above the SD range indicated progressive disease (PD). Comparison was made to tumor response classification according to percentage change in the lesion’s maximal diameter per RECIST. Lin’s concordance correlation coefficient, Bland–Altman plot, Wilcoxon signed rank test, and Student t test were used for analysis. Significance was set at 0.05.
Results
RDT range for SD ranged from −0.46 to +2.17. Six lesions with PR based on RECIST showed PR based on their volumetric growth rate (mean RDT of −17.3 ± 2.6). Similarly, one lesion with PD according to RECIST was categorized as PD based on its growth kinetics (RDT of 10.2). However, 14 (51.85%) lesions classified as SD by RECIST had PR according to growth kinetics (mean RDT of −7.8), six (22.22%) lesions were categorized as SD (mean RDT of 0.8), whereas seven (25.93%) lesions showed PD (mean RDT of 4.5). Growth kinetic parameters were significantly different for lesions with PR when compared to lesions with PD ( P < .0001).
Conclusions
In patients with breast cancer liver metastases undergoing locoregional therapy, RECIST categorization may not be an accurate reflection of treatment response.
Metastatic breast cancer is not considered a curable disease at present and accounts for most deaths associated with breast cancer . About 40%–50% of all patients diagnosed with breast cancer will develop liver metastasis during the course of their illness , but rarely (5% of cases) liver-only metastatic involvement can be seen . Management of liver metastases from breast cancer relies heavily on systemic therapies . Locoregional treatments are also available as adjuncts including surgical resection of liver metastases , local ablation , chemoembolization, transarterial chemoembolization, transarterial radioembolization (TARE) , and stereotactic body radiotherapy . Surgical resection of liver metastasis is performed in carefully selected patients and because only 10%–20% of patients are surgical candidates, alternatives must be considered. TARE with yttrium-90 ( 90 Y) is an effective alternative and has been successfully used for treatment of liver metastases in patients with chemorefractory breast cancer. Median overall survival in patients with breast cancer liver metastases undergoing treatment with 90 Y was recently reported at 11.5 months . Because of relatively poorer prognosis and shorter survival in patients with breast cancer liver metastases, there is a need for effective early response assessment to locoregional therapies.
Currently, Response Evaluation Criteria in Solid Tumors (RECIST) 1.1 is the commonly used treatment response evaluation tool in clinical cancer trials involving patients with metastatic breast cancer but has several limitations. First, RECIST are based on an assumption that tumors are spherical and change proportionally in response to treatment; however, some studies have shown that tumors may have irregular shape and nonspherical morphologies rendering RECIST unreliable . Second, novel locoregional therapies may induce changes in certain morphologic characteristics (density, necrosis, tumor margins, and so forth) of the tumor with or without any appreciable change in its size . RECIST are unable to account for these changes preventing it from assessing response accurately in such scenarios. This has led to the development of certain tumor and therapy specific criteria, which provide better depiction of response . Third, RECIST guideline categorizes treatment response as stable disease (SD) despite up to 30% decrease or 20% increase in tumor size. Therefore, it will be impossible to accurately assess response to novel locoregional treatments, which may cause clinically significant changes in tumors without crossing the thresholds drawn by RECIST.
Get Radiology Tree app to read full this article<
Methods and materials
Get Radiology Tree app to read full this article<
Patient Cohort
Patient selection
Get Radiology Tree app to read full this article<
TARE with 90 Y microspheres
Get Radiology Tree app to read full this article<
MDCT Imaging Protocol
Get Radiology Tree app to read full this article<
Imaging Evaluation
Lesion selection
Get Radiology Tree app to read full this article<
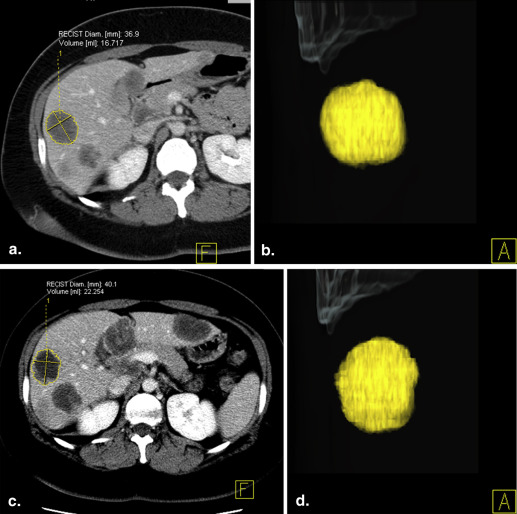
Tumor volumetry
Get Radiology Tree app to read full this article<
Calculation of Doubling Time and Reciprocal of Doubling Time
Get Radiology Tree app to read full this article<
DT=Δtlog2/(logV2−logV1), DT
=
Δ
t
log
2
/
(
log
V
2
−
log
V
1
)
,
where V 1 is volume of the lesion in the baseline study, V 2 is volume of the lesion in the follow-up study, and Δ t is the interval between the studies. As DT is an exponential function without normal distribution, reciprocal of DT (RDT) was calculated using the formula:
RDT=365/DT, RDT
=
365
/
DT
,
thus providing a linear representation of tumor growth rate . RDT is the number of times in a year that the tumor volume doubles and is dimensionless. RDT value of zero indicates no change in tumor size, a negative value indicates a decrease in size of the tumor, and a positive value shows tumor growth.
Get Radiology Tree app to read full this article<
Objective Response Assessment (RECIST 1.1)
Get Radiology Tree app to read full this article<
Treatment Response Based on Volumetric Growth Rate
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
ΔV=V−VT. Δ
V
=
V
−
V
T
.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
ΔV=(ΔV1)2+(ΔV2)2−−−−−−−−−−−−−√. Δ
V
=
(
Δ
V
1
)
2
+
(
Δ
V
2
)
2
.
Replacing the values for ΔV1 Δ
V
1 and ΔV2 Δ
V
2 , Equation (1) can be written as
100%ΔV=p(V1)2+(V2)2−−−−−−−−−−−√. 100
%
Δ
V
=
p
(
V
1
)
2
+
(
V
2
)
2
.
Therefore, using Equation (2), we can write the conditions of measurement accuracy (V1−V2>ΔV) (
V
1
−
V
2
Δ
V
) as
100%|V1−V2|(V1)2+(V2)2√>p, 100
%
|
V
1
−
V
2
|
(
V
1
)
2
+
(
V
2
)
2
p
,
where p = 7.87% and determines the boundaries of SD, in a similar approach as WHO guidelines and RECIST.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
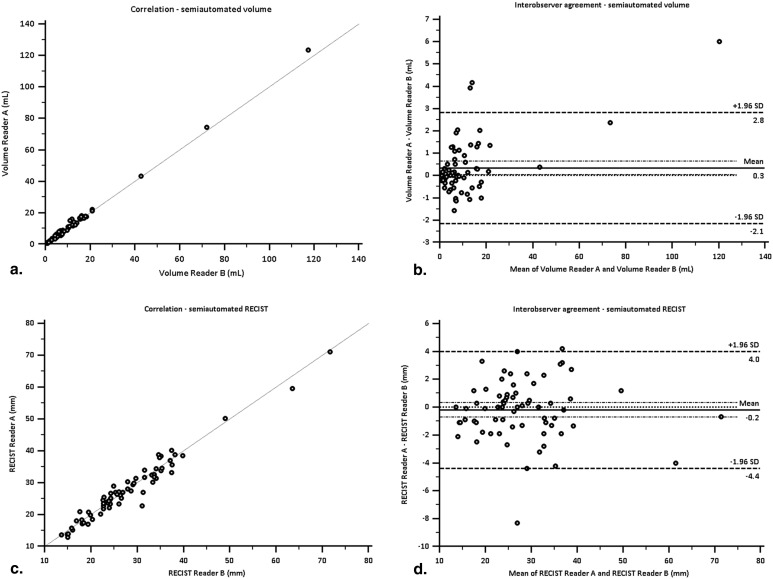
Assessment of Interobserver Reproducibility
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Demographics
Get Radiology Tree app to read full this article<
Objective Response Assessment (RECIST 1.1) and Classification of Treatment Response
Get Radiology Tree app to read full this article<
Classification of Treatment Response Based on Volumetric Growth Rate
Get Radiology Tree app to read full this article<
Comparative Analysis: RECIST 1.1 Versus Volumetric Growth Rate
Get Radiology Tree app to read full this article<
Table 1
Characteristics of Lesions Classified as SD by RECIST 1.1
Lesions Interscan Interval (days) RECIST Change (%) RECIST Class Volume Change (%) DT (days) RDT Response according to RDT 1 56 −18.80 SD −78.20 −25.48 −14.32 PR 2 48 −28.1 SD −69.68 −27.88 −13.09 PR 3 48 −29.44 SD −67.80 −29.36 −12.43 PR 4 42 −22.22 SD −60.21 −31.59 −11.55 PR 5 22 −19.83 SD −36.01 −34.15 −10.69 PR 6 43 −13.22 SD −53.46 −38.97 −9.37 PR 7 52 −6.83 SD −59.70 −39.66 −9.20 PR 8 36 −6.70 SD −40.62 −47.87 −7.62 PR 9 34 −7.06 SD −27.81 −72.33 −5.05 PR 10 58 −12.35 SD −36.26 −89.27 −4.09 PR 11 27 −6.49 SD −15.77 −109.08 −3.35 PR 12 34 −8.38 SD −18.38 −116.06 −3.14 PR 13 52 −10.76 SD −25.46 −122.65 −2.98 PR 14 35 −1.12 SD −14.83 −151.17 −2.41 PR 15 28 −2.90 SD −2.40 −798.09 −0.46 SD 16 27 4.11 SD 0.33 5736.48 0.06 SD 17 39 −2.79 SD 5.93 469.08 0.78 SD 18 24 11.16 SD 4.57 372.61 0.98 SD 19 43 10.23 SD 10.64 294.68 1.24 SD 20 22 1.51 SD 9.48 168.41 2.17 SD 21 30 19.28 SD 13.44 164.86 2.21 PD 22 36 4.73 SD 27.21 103.67 3.52 PD 23 36 4.28 SD 27.68 102.13 3.57 PD 24 28 9.96 SD 25.21 86.34 4.23 PD 25 51 8.39 SD 52.26 84.09 4.34 PD 26 51 16.02 SD 64.23 71.26 5.12 PD 27 51 10.71 SD 125.27 43.53 8.39 PD
DT, doubling time; PD, progressive disease; PR, partial response; RDT, reciprocal of doubling time; RECIST, Response Evaluation Criteria in Solid Tumors; SD, stable disease.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Interobserver Reproducibility and Agreement
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
References
1. Diamond J.R., Finlayson C.A., Borges V.F.: Hepatic complications of breast cancer. Lancet Oncol 2009; 10: pp. 615-621.
2. Kostov D.V., Kobakov G.L., Yankov D.V.: Prognostic factors related to surgical outcome of liver metastases of breast cancer. J Breast Cancer 2013; 16: pp. 184-192.
3. Bangash A.K., Atassi B., Kaklamani V., et. al.: 90Y radioembolization of metastatic breast cancer to the liver: toxicity, imaging response, survival. J Vasc Interv Radiol 2007; 18: pp. 621-628.
4. O’Reilly S.M., Richards M.A., Rubens R.D.: Liver metastases from breast cancer: the relationship between clinical, biochemical and pathological features and survival. Eur J Cancer 1990; 26: pp. 574-577.
5. Diaz R., Santaballa A., Munarriz B., et. al.: Hepatic resection in breast cancer metastases: should it be considered standard treatment?. Breast 2004; 13: pp. 254-258.
6. Come S.E., Borges V.F.: Role of fulvestrant in sequential hormonal therapy for advanced, hormone receptor-positive breast cancer in postmenopausal women. Clin Breast Cancer 2005; 6: pp. S15-S22.
7. d’Annibale M., Piovanello P., Cerasoli V., et. al.: Liver metastases from breast cancer: the role of surgical treatment. Hepatogastroenterology 2005; 52: pp. 1858-1862.
8. Bortolotto C., Macchi S., Veronese L., et. al.: Radiofrequency ablation of metastatic lesions from breast cancer. J Ultrasound 2012; 15: pp. 199-205.
9. Cianni R., Pelle G., Notarianni E., et. al.: Radioembolisation with (90)Y-labelled resin microspheres in the treatment of liver metastasis from breast cancer. Eur Radiol 2013; 23: pp. 182-189.
10. Adam R.: Chemotherapy and surgery: new perspectives on the treatment of unresectable liver metastases. Ann Oncol 2003; 14: pp. ii13-ii16.
11. Eisenhauer E.A., Therasse P., Bogaerts J., et. al.: New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer 2009; 45: pp. 228-247.
12. Suzuki C., Blomqvist L., Hatschek T., et. al.: Impact of the first tumor response at eight weeks on overall survival in metastatic breast cancer patients treated with first-line combination chemotherapy. Med Oncol 2013; 30: pp. 415.
13. Galizia M.S., Tore H.G., Chalian H., et. al.: Evaluation of hepatocellular carcinoma size using two-dimensional and volumetric analysis: effect on liver transplantation eligibility. Acad Radiol 2011; 18: pp. 1555-1560.
14. Rezai P., Mulcahy M.F., Tochetto S.M., et. al.: Morphological analysis of pancreatic adenocarcinoma on multidetector row computed tomography: implications for treatment response evaluation. Pancreas 2009; 38: pp. 799-803.
15. Chun Y.S., Vauthey J.N., Boonsirikamchai P., et. al.: Association of computed tomography morphologic criteria with pathologic response and survival in patients treated with bevacizumab for colorectal liver metastases. JAMA 2009; 302: pp. 2338-2344.
16. Shindoh J., Chun Y.S., Loyer E.M., et. al.: Non-size-based response criteria to preoperative chemotherapy in patients with colorectal liver metastases: the morphologic response criteria. Curr Colorectal Cancer Rep 2013; 9: pp. 198-202.
17. Choi H., Charnsangavej C., Faria S.C., et. al.: Correlation of computed tomography and positron emission tomography in patients with metastatic gastrointestinal stromal tumor treated at a single institution with imatinib mesylate: proposal of new computed tomography response criteria. J Clin Oncol 2007; 25: pp. 1753-1759.
18. Mehrara E., Forssell-Aronsson E., Ahlman H., et. al.: Quantitative analysis of tumor growth rate and changes in tumor marker level: specific growth rate versus doubling time. Acta Oncol 2009; 48: pp. 591-597.
19. Schwartz M.: A biomathematical approach to clinical tumor growth. Cancer 1961; 14: pp. 1272-1294.
20. Rezai P., Yaghmai V., Tochetto S.M., et. al.: Change in the growth rate of localized pancreatic adenocarcinoma in response to gemcitabine, bevacizumab, and radiation therapy on MDCT. Int J Radiat Oncol Biol Phys 2011; 81: pp. 452-459.
21. Salem R., Thurston K.G.: Radioembolization with 90Yttrium microspheres: a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies. Part 1: Technical and methodologic considerations. J Vasc Interv Radiol 2006; 17: pp. 1251-1278.
22. Sato K.T., Lewandowski R.J., Mulcahy M.F., et. al.: Unresectable chemorefractory liver metastases: radioembolization with 90Y microspheres—safety, efficacy, and survival. Radiology 2008; 247: pp. 507-515.
23. Therasse P., Arbuck S.G., Eisenhauer E.A., et. al.: New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J Natl Cancer Inst 2000; 92: pp. 205-216.
24. Kuhnigk J.M., Dicken V., Bornemann L., et. al.: Morphological segmentation and partial volume analysis for volumetry of solid pulmonary lesions in thoracic CT scans. IEEE Trans Med Imaging 2006; 25: pp. 417-434.
25. Moltz J.H., Bornemann L., Kuhnigk J.-M., et. al.: Advanced segmentation techniques for lung nodules, liver metastases, and enlarged lymph nodes in CT scans. IEEE J Sel Top Signal Process 2009; 3: pp. 122-134.
26. Keil S., Behrendt F.F., Stanzel S., et. al.: Semi-automated measurement of hyperdense, hypodense and heterogeneous hepatic metastasis on standard MDCT slices. Comparison of semi-automated and manual measurement of RECIST and WHO criteria. Eur Radiol 2008; 18: pp. 2456-2465.
27. Zhang J., Kang S.K., Wang L., et. al.: Distribution of renal tumor growth rates determined by using serial volumetric CT measurements. Radiology 2009; 250: pp. 137-144.
28. Honda O., Johkoh T., Sekiguchi J., et. al.: Doubling time of lung cancer determined using three-dimensional volumetric software: comparison of squamous cell carcinoma and adenocarcinoma. Lung Cancer 2009; 66: pp. 211-217.
29. Keil S., Plumhans C., Behrendt F.F., et. al.: Semi-automated quantification of hepatic lesions in a phantom. Invest Radiol 2009; 44: pp. 82-88.
30. Taylor J.: An introduction to error analysis. The study of uncertainties in physical measurements.1997.University Science BooksSausalito, CA
31. Mantatzis M., Kakolyris S., Amarantidis K., et. al.: Treatment response classification of liver metastatic disease evaluated on imaging. Are RECIST unidimensional measurements accurate?. Eur Radiol 2009; 19: pp. 1809-1816.
32. Gonzalez-Guindalini F.D., Botelho M.P., Harmath C.B., et. al.: Assessment of liver tumor response to therapy: role of quantitative imaging. Radiographics 2013; 33: pp. 1781-1800.
33. Yaghmai V., Miller F.H., Rezai P., et. al.: Response to treatment series: part 2, tumor response assessment—using new and conventional criteria. AJR Am J Roentgenol 2011; 197: pp. 18-27.
34. Curran S.D., Muellner A.U., Schwartz L.H.: Imaging response assessment in oncology. Cancer Imaging 2006; 6: pp. S126-S130.
35. Edeline J., Boucher E., Rolland Y., et. al.: Comparison of tumor response by Response Evaluation Criteria in Solid Tumors (RECIST) and modified RECIST in patients treated with sorafenib for hepatocellular carcinoma. Cancer 2012; 118: pp. 147-156.
36. Weng Z., Ertle J., Zheng S., et. al.: Choi criteria are superior in evaluating tumor response in patients treated with transarterial radioembolization for hepatocellular carcinoma. Oncol Lett 2013; 6: pp. 1707-1712.
37. Tochetto S.M., Rezai P., Rezvani M., et. al.: Does multidetector CT attenuation change in colon cancer liver metastases treated with 90Y help predict metabolic activity at FDG PET?. Radiology 2010; 255: pp. 164-172.
38. Wulff A.M., Bolte H., Fischer S., et. al.: Lung, liver and lymph node metastases in follow-up MSCT: comprehensive volumetric assessment of lesion size changes. Rofo 2012; 184: pp. 820-828.
39. Smits M.L., Prince J.F., Rosenbaum C.E., et. al.: Intra-arterial radioembolization of breast cancer liver metastases: a structured review. Eur J Pharmacol 2013; 709: pp. 37-42.
40. Miller F.H., Keppke A.L., Reddy D., et. al.: Response of liver metastases after treatment with yttrium-90 microspheres: role of size, necrosis, and PET. AJR Am J Roentgenol 2007; 188: pp. 776-783.