
Rationale and Objectives
To compare quality of ultra-low-dose thin-section computed tomography (CT) images of the lung reconstructed using model-based iterative reconstruction (MBIR) and adaptive statistical iterative reconstruction (ASIR) to filtered back projection (FBP) and to determine the minimum tube current–time product on MBIR images by comparing to standard-dose FBP images.
Materials and Methods
Ten cadaveric lungs were scanned using 120 kVp and four different tube current–time products (8, 16, 32, and 80 mAs). Thin-section images were reconstructed using MBIR, three ASIR blends (30%, 60%, and 90%), and FBP. Using the 8-mAs data, side-to-side comparison of the four iterative reconstruction image sets to FBP was performed by two independent observers who evaluated normal and abnormal findings, subjective image noise, streak artifact, and overall image quality. Image noise was also measured quantitatively. Subsequently, 8-, 16-, and 32-mAs MBIR images were compared to standard-dose FBP images. Comparisons of image sets were analyzed using the Wilcoxon signed rank test with Bonferroni correction.
Results
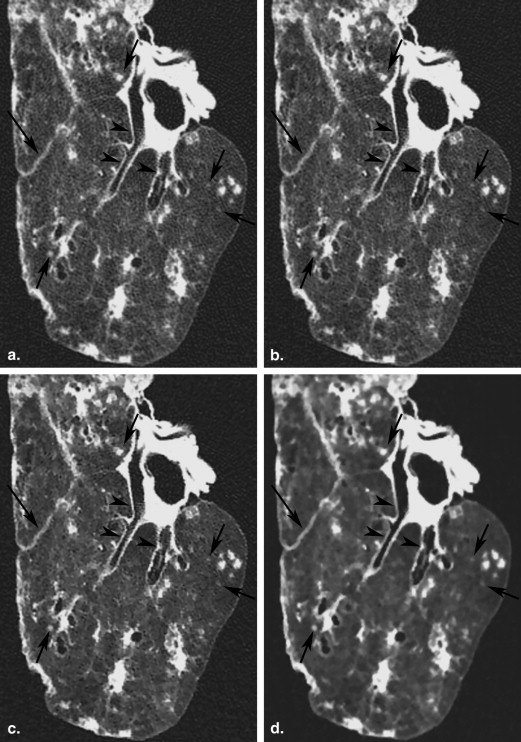
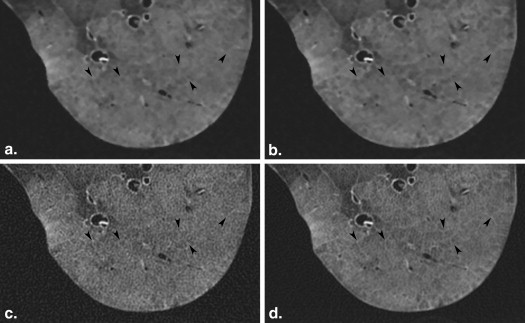
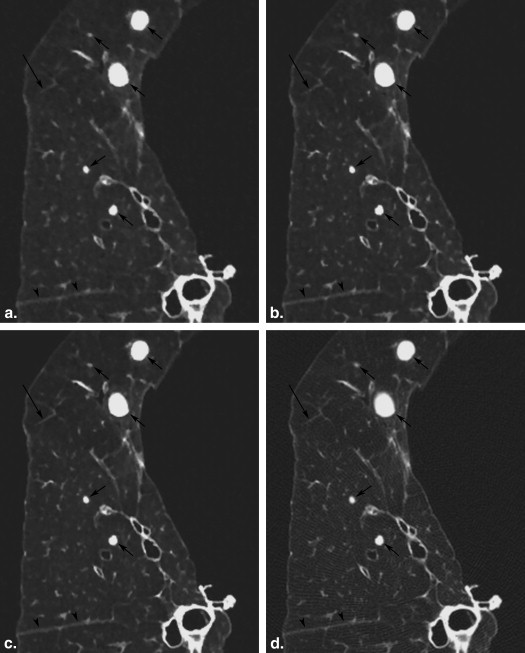
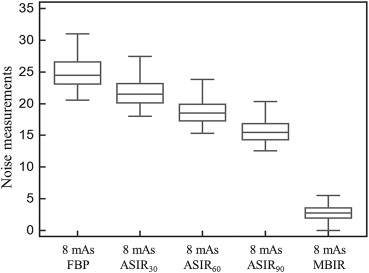
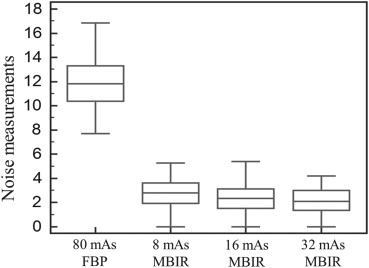
At 8 mAs, MBIR images were significantly better ( P < .005) than other reconstruction techniques except in evaluation of interlobular septal thickening. Each set of low-dose MBIR images had significantly lower ( P < .001) subjective and objective noise and streak artifacts than standard-dose FBP images. Conspicuity and visibility of normal and abnormal findings were not significantly different between 16-mAs MBIR and 80-mAs FBP images except in identification of intralobular reticular opacities.
Conclusions
MBIR imaging shows higher overall quality with lower noise and streak artifacts than ASIR or FBP imaging, resulting in nearly 80% dose reduction without any degradations of overall image quality.
The increase of the radiation dose delivered in computed tomography (CT) has recently been a problem. Because there is a trade-off between image quality and radiation dose on CT, however, it is not always appropriate to decrease radiation dose on CT. Iterative reconstruction algorithms for CT have been developed by multiple equipment manufacturers to reduce image noise associated with radiation dose reduction . Adaptive statistical iterative reconstruction (ASIR) and model-based iterative reconstruction (MBIR) are types of iterative reconstruction algorithms available on clinical settings. The ASIR technique models photon and electronic noise statistics; by partially correcting for fluctuations in projection measurements due to limited photon statistics, ASIR enables a time-efficient reduction in pixel variance that is statistically unlikely to be representative of anatomic features resulting in a reduction of image noise with no decrement in spatial resolution . In clinical practice, ASIR is typically used in combination with the standard filtered back projection (FBP) reconstruction to create blended images. As compared to ASIR, MBIR is a more mathematically complex and time-consuming technique as it models not only system statistics but also system optics . Phantom experiments show that MBIR has potential to improve spatial resolution and allow further reductions in image noise . To date, few studies have evaluated CT image quality of the lung using MBIR . Thus, unlike FBP and ASIR, MBIR technique might have the potential not to degrade image quality even under the extreme dose reduction. McCollough et al. reported that the advances in data acquisition, image reconstruction, and optimization processes that were identified by consensus as being necessary to achieve submillisievert-dose CT examinations. It is expected that MBIR might be one of techniques to enable a submillisievert-dose CT. The present study was performed using cadaveric lung models that can provide multiple acquisitions to determine the minimum tube current–time product at which image quality of a low-dose MBIR study is comparable to that of a standard-dose FBP study. The aim of this present study was two-fold: to compare quality of ultra-low-dose thin-section CT images of the lung reconstructed using MBIR and ASIR to FBP and to determine the minimum tube current–time product at which image quality of an MBIR study is comparable to that of a standard-dose FBP.
Materials and methods
Cadaveric Lungs and Imaging
We obtained approval from our internal Ethics Review Board. Informed consent was obtained for the use of patient biomaterial and for retrospective review of patient records and images. Ten cadaveric lungs were inflated and fixed by the method of Heitzman . These lungs were distended through the main bronchus with fixative fluid that contained polyethylene glycol 400, 95% ethyl alcohol, 40% formalin, and water in the proportions of 10:5:2:3. The specimens were immersed in fixative for 2 days and the lungs were then air dried. The pathologic diagnoses of these 10 lungs were usual interstitial pneumonia ( n = 1), diffuse alveolar damage ( n = 1), diffuse panbronchiolitis ( n = 1), pneumonia ( n = 2), emphysema ( n = 1), diffuse alveolar hemorrhage ( n = 1), metastatic disease ( n = 2), and lymphangitic carcinomatosis ( n = 1).
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Subjective Image Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Objective Image Analysis
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Radiation Doses
Get Radiology Tree app to read full this article<
Table 1
Radiation Dose Descriptions
Low Dose Standard Dose 8 mAs 16 mAs 32 mAs 80 mAs CTDIvol (mGy) 0.65 1.30 2.59 6.49 DLP (mGy-cm) 22.15 44.30 88.60 221.50 ED (mSv) 0.31 0.62 1.24 3.10
CTDIvol, computed tomography dose index volume; DLP, dose–length product; ED, effective dose.
Get Radiology Tree app to read full this article<
Subjective Evaluation of CT Findings
Get Radiology Tree app to read full this article<
Table 2
Comparison among FBP, ASIR, and MBIR on Ultra-low-dose (8 mAs) CT
Normal Findings Abnormal Findings Other Findings Overall Image Quality Central Vessels and Airways Peripheral Vessels and Airways Interlobar Fissures Nodules GGO ISP Image Noise Streak Artifact Reconstruction technique MBIR 4.83 ± 0.07 4.68 ± 0.09 4.75 ± 0.11 4.96 ± 0.04 4.84 ± 0.07 4.19 ± 0.16 5.00 ± 0.00 5.00 ± 0.00 4.97 ± 0.03 ASIR 90 4.06 ± 0.11 4.04 ± 0.07 4.00 ± 0.13 4.00 ± 0.05 4.16 ± 0.07 3.88 ± 0.09 4.21 ± 0.07 4.03 ± 0.12 4.55 ± 0.09 ASIR 60 3.52 ± 0.09 3.32 ± 0.09 3.19 ± 0.10 3.39 ± 0.09 3.84 ± 0.07 3.31 ± 0.12 3.73 ± 0.08 3.45 ± 0.09 3.55 ± 0.09 ASIR 30 3.00 ± 0.00 3.00 ± 0.00 3.00 ± 0.00 3.04 ± 0.04 3.04 ± 0.04 3.00 ± 0.00 3.03 ± 0.03 3.00 ± 0.00 3.00 ± 0.00 FBP 3.00 ± 0.00 3.00 ± 0.00 3.00 ± 0.00 3.00 ± 0.00 3.00 ± 0.00 3.00 ± 0.00 3.00 ± 0.00 3.00 ± 0.00 3.00 ± 0.00 Pairwise comparison ( P *) MBIR versus ASIR 90 <.001 <.001 .005 <.001 <.001 .962 <.001 <.001 <.001 ASIR 60 <.001 <.001 <.001 <.001 <.001 .002 <.001 <.001 <.001 ASIR 30 <.001 <.001 <.001 <.001 <.001 <.001 <.001 <.001 <.001 FBP <.001 <.001 <.001 <.001 <.001 <.001 <.001 <.001 <.001 ASIR 90 versus ASIR 60 <.001 <.001 <.001 <.001 .084 .005 <.001 <.001 <.001 ASIR 30 <.001 <.001 <.001 <.001 <.001 <.001 <.001 <.001 <.001 FBP <.001 <.001 <.001 <.001 <.001 <.001 <.001 <.001 <.001 ASIR 60 versus ASIR 30 <.001 .026 .825 .006 <.001 .197 <.001 <.001 <.001 FBP <.001 .026 .825 .003 <.001 .197 <.001 <.001 <.001 ASIR 30 versus FBP 1.000 1.000 1.000 1.000 1.000 1.000 1.000 1.000 1.000
ASIR, adaptive statistical iterative reconstruction; GGO, ground-glass opacity; ISP, interlobular septal thickening; FBP, filtered back projection; MBIR, model-based iterative reconstruction.
Data are presented as mean ± standard deviation. Data of the subjective image analysis were statistically analyzed using the Wilcoxon signed rank tests with a Bonferroni correction applied for multiple comparisons. P \* is a Bonferroni-corrected P value. P \* value <.05 was considered to be significant.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 3
Comparison between 8-mAs, 16-mAs, and 32-mAs MBIR Versus 80-mAs FBP
Normal Findings Abnormal Findings Other Findings Overall Image Quality Central Vessels and Airways Peripheral Vessels and Airways Interlobar Fissures Nodules GGO ISP Image Noise Streak Artifact Reconstruction technique 32-mAs MBIR 3.33 ± 0.09 3.50 ± 0.11 3.53 ± 0.17 3.46 ± 0.09 3.77 ± 0.11 3.44 ± 0.13 4.97 ± 0.03 4.97 ± 0.03 3.67 ± 0.12 16-mAs-MBIR 3.07 ± 0.07 3.14 ± 0.14 3.27 ± 0.12 3.18 ± 0.10 3.27 ± 0.13 2.75 ± 0.17 4.93 ± 0.05 4.93 ± 0.05 2.93 ± 0.08 8-mAs MBIR 3.07 ± 0.07 2.73 ± 0.18 2.93 ± 0.07 2.82 ± 0.12 2.86 ± 0.12 2.19 ± 0.10 4.87 ± 0.06 4.93 ± 0.05 2.63 ± 0.10 80-mAs FBP 3.00 ± 0.00 3.00 ± 0.00 3.00 ± 0.00 3.00 ± 0.00 3.00 ± 0.00 3.00 ± 0.00 3.00 ± 0.00 3.00 ± 0.00 3.00 ± 0.00 Pairwise comparison ( P *) 32-mAs MBIR versus 16-mAs MBIR .179 .047 .243 .108 .005 .002 1.000 1.000 <.001 8-mAs MBIR .179 <.001 .015 .001 <.001 <.001 1.000 1.000 <.001 80-mAs FBP .004 .001 .037 <.001 <.001 .023 <.001 <.001 <.001 16-mAs MBIR versus 8-mAs MBIR 1.000 .023 .115 .013 .023 .017 .965 1.000 .028 80-mAs FBP 1.000 1.000 .243 .576 .333 .983 <.001 <.001 1.000 8-mAs MBIR versus 80-mAs FBP 1.000 .821 1.000 .805 1.000 <.001 <.001 <.001 .007
ASIR, adaptive statistical iterative reconstruction; GGO, ground-glass opacity; ISP, interlobular septal thickening; FBP, filtered back projection; MBIR, model-based iterative reconstruction.
Data are presented as mean ± standard deviation. Data of the subjective image analysis were statistically analyzed using the Wilcoxon signed rank tests with a Bonferroni correction applied for multiple comparisons. P \* is a Bonferroni-corrected P value. P \* value <0.05 was considered to be significant.
Get Radiology Tree app to read full this article<
Quantitative Image Noise Measurements
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Prakash P., Kalra M.K., Kambadakone A.K., et. al.: Reducing abdominal CT radiation dose with adaptive statistical iterative reconstruction technique. Invest Radiol 2010; 45: pp. 202-210.
2. Singh S., Kalra M.K., Hsieh J., et. al.: Abdominal CT: comparison of adaptive statistical iterative and filtered back projection reconstruction techniques. Radiology 2010; 257: pp. 373-383.
3. Honda O., Yanagawa M., Inoue A., et. al.: Image quality of multiplanar reconstruction of pulmonary CT scans using adaptive statistical iterative reconstruction. Br J Radiol 2011; 84: pp. 335-341.
4. Gervaise A., Osemont B., Lecocq S., et. al.: CT image quality improvement using Adaptive Iterative Dose Reduction with wide-volume acquisition on 320-detector CT. Eur Radiol 2012; 22: pp. 295-301.
5. Prakash P., Kalra M.K., Ackman J.B., et. al.: Diffuse lung disease: CT of the chest with adaptive statistical iterative reconstruction technique. Radiology 2010; 256: pp. 261-269.
6. Singh S., Kalra M.K., Gilman M.D., et. al.: Adaptive statistical iterative reconstruction technique for radiation dose reduction in chest CT: a pilot study. Radiology 2011; 259: pp. 565-573.
7. Funama Y., Taguchi K., Utsunomiya D., et. al.: Combination of a low-tube-voltage technique with hybrid iterative reconstruction (iDose) algorithm at coronary computed tomographic angiography. J Comput Assist Tomogr 2011; 35: pp. 480-485.
8. Moscariello A., Takx R.A., Schoepf U.J., et. al.: Coronary CT angiography: image quality, diagnostic accuracy, and potential for radiation dose reduction using a novel iterative image reconstruction technique-comparison with traditional filtered back projection. Eur Radiol 2011; 21: pp. 2130-2138.
9. Thibault J.B., Sauer K.D., Bouman C.A., et. al.: A three-dimensional statistical approach to improved image quality for multislice helical CT. Med Phys 2007; 34: pp. 4526-4544.
10. Katsura M., Matsuda I., Akahane M., et. al.: Model-based iterative reconstruction technique for radiation dose reduction in chest CT: comparison with the adaptive statistical iterative reconstruction technique. Eur Radiol 2012; 22: pp. 1613-1623.
11. Katsura M., Matsuda I., Akahane M., et. al.: Model-based iterative reconstruction technique for ultralow-dose chest CT: comparison of pulmonary nodule detectability with the adaptive statistical iterative reconstruction technique. Invest Radiol 2013; 48: pp. 206-212.
12. Yamada Y., Jinzaki M., Tanami Y., et. al.: Model-based iterative reconstruction technique for ultralow-dose computed tomography of the lung: a pilot study. Invest Radiol 2012; 47: pp. 482-489.
13. Vardhanabhuti V., Loader R.J., Mitchell G.R., et. al.: Image quality assessment of standard- and low-dose chest CT using filtered back projection, adaptive statistical iterative reconstruction, and novel model-based iterative reconstruction algorithms. AJR Am J Roentgenol 2013; 200: pp. 545-552.
14. Neroladaki A., Botsikas D., Boudabbous S., et. al.: Computed tomography of the chest with model-based iterative reconstruction using a radiation exposure similar to chest X-ray examination: preliminary observations. Eur Radiol 2013; 23: pp. 360-366.
15. McCollough C.H., Chen G.H., Kalender W., et. al.: Achieving routine submillisievert CT scanning: report from the summit on management of radiation dose in CT. Radiology 2012; 264: pp. 567-580.
16. Markarian B., Dailey E.T.: Preparation of inflated lung specimens.Groskin S.A.Heitzman’s The lung: radiologic-pathologic correlations.1993.MosbySt. Louis:pp. 4-12.
17. Aberle D.R., Berg C.D., Black W.C., et. al.: The National Lung Screening Trial: overview and study design. Radiology 2011; 258: pp. 243-253.
18. Boehm T., Willmann J.K., Hilfiker P.R., et. al.: Thin-section CT of the lung: dose electrocardiographic triggering influence diagnosis?. Radiology 2003; 229: pp. 483-491.
19. Goldman L.W.: Principles of CT: radiation dose and image quality. J Nucl Med Technol 2007; 35: pp. 213-225.
20. American Association of Physicists in Medicine. The measurement, reporting, and management of radiation dose in CT; 2008. Available at: http://www.aapm.org/pubs/reports/rpt_96.pdf . Accessed January 15, 2012.
21. Marin D., Nelson R.C., Schindera S.T., et. al.: Low-tube-voltage, high-tube-current multidetector abdominal CT: improved image quality and decreased radiation dose with adaptive statistical iterative reconstruction algorithm—initial clinical experience. Radiology 2010; 254: pp. 145-153.
22. Yanagawa M., Honda O., Yoshida S., et. al.: Adaptive statistical iterative reconstruction technique for pulmonary CT: image quality of the cadaveric lung on standard- and reduced-dose CT. Acad Radiol 2010; 17: pp. 1259-1266.
23. Hara A.K., Paden R.G., Silva A.C., et. al.: Iterative reconstruction technique for reducing body radiation dose at CT: feasibility study. AJR Am J Roentgenol 2009; 193: pp. 764-771.
24. Yu Z., Thibault J.B., Bouman C.A., et. al.: Fast model-based X-ray CT reconstruction using spatially nonhomogeneous ICD optimization. IEEE Trans Image Process 2011; 20: pp. 161-175.
25. Wall B.F., Hart D.: Revised radiation doses for typical X-ray examinations. Report on a recent review of doses to patients from medical X-ray examinations in the UK by NRPB. National Radiological Protection Board. Br J Radiol 1997; 70: pp. 437-439.