
Rationale and Objectives
The aims of this study were to investigate the value of ultrasound elastography (UE) in the diagnosis of lymphadenopathy and to explore whether UE could improve the differentiation between benign and malignant cervical lymph nodes (LNs).
Materials and Methods
B-mode ultrasound, power Doppler imaging, and UE were performed in 107 consecutive patients with 128 cervical LNs. Only LNs that unequivocally matched between sonography and pathology were analyzed. The results of B-mode ultrasound, power Doppler imaging, and UE were interpreted separately to assess cervical LNs, using histopathologic analysis as the reference standard.
Results
A marked difference ( P = .000) was found in the strain ratio between 70 malignant LNs (median, 2.71; range, 1.36–36.09) and 58 benign LNs (median, 1.44; range, 0.62–3.90). Receiver-operating characteristic curves showed that a strain ratio > 1.5 had high utility in enlarged cervical LN classification, with 92.5% sensitivity, 53.4% specificity, and a Youden’s index of 0.463. These results were significantly better than those obtained using the best grayscale criterion, a ratio of long-axis to short-axis diameter > 2, which yielded 58.6% sensitivity, 70% specificity, and a Youden’s index of 0.286. The κ values for interobserver agreement were highest using UE, at 0.881 (observer 1 vs observer 2), 0.828 (observer 1 vs observer 3), and 0.946 (observer 2 vs observer 3).
Conclusions
UE as an adjunct ultrasound modality holds some promise in screening and monitoring lymphadenopathy.
To date, open cervical lymph node (LN) biopsy combined with pathologic examination remains the gold standard to determine whether LNs metastasize . However, the procedure can alter patterns of lymphatic drainage for up to 1 year following surgery and may portend a poor prognosis, especially for patients to present late to the hospital . Fine-needle aspiration cytology has proven to be an efficient tool for diagnosis, but it is an invasive approach and is subject to sampling and analytic uncertainty. Thus, improved and more reliable criteria for determining which nodules should be followed up and which should be aspirated are needed . In response, significant research efforts have been directed toward identification using noninvasive methods for diagnosing enlarged LNs. This technique must be safe, accurate, and accessible, like many standard medical screening tests.
Ultrasonography, compared to computed tomography and magnetic resonance imaging, has proven to be a valuable tool for the detection of LNs, but making a clear differentiation between benign nodal diseases and malignant lymphadenopathy remains difficult. Recently, ultrasound elastography (UE) has been presented as a novel technique to aid cancer research. It can be superimposed during B-mode ultrasound (B-US) examination to assess and measure tissue elasticity.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Patients, Procedure, and Examination Technique
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Ultrasound, PDI, and UE Evaluation
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Pathologic Examination
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
B-US
Get Radiology Tree app to read full this article<
Table 1
The P Value of X2 Test of the Ultrasonographic Indexes of Lymph Nodes
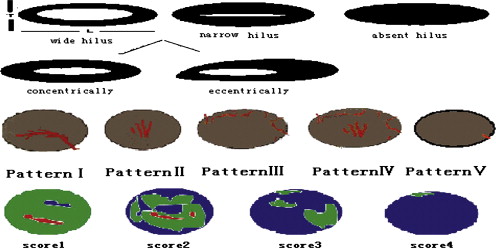
L/T Hilum PDI Pattern UE Score Strain Ratio Sonomor-phologic features ≥2 <2 Normal ∗ Abnormal † I or V II, III, or IV 1or 2 3or 4 ≤1.5 >1.5 Benign 37 (28.9%) 21 (16.4%) 14 (10.9%) 44 (34.3%) 45 (35.2%) 13 (10.2%) 51 (39.8%) 7 (5.5%) 31 (24.2%) 27 (21.1%) Malignant 21 (16.4%) 49 (38.3%) 4 (3.1%) 66 (51.6%) 4 (3.1%) 66 (51.6%) 35 (27.3%) 35 (27.3%) 5 (3.9%) 65 (50.8%)P .000 .003 .000 .000 .000 Contingency coefficient 0.320 0.255 0.593 0.373 0.456 Odds ratio (95% confidence interval) 4.111 (1.961–8.619) 5.250 (1.622–16.998) 57.115 (17.498–186.429) 7.286 (2.908–18.254) 10.230 (5.245–42.472)
L/T, ratio of long-axis to short-axis diameter; PDI, power Doppler imaging; UE, ultrasound elastography.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
PDI
Get Radiology Tree app to read full this article<
Table 2
Comparison of Sensitivity, Specificity, Accuracy for B- US, PDI, and UE
Imaging Modality Sensitivity Specificity Accuracy PPV NPV Youden’s Index (Sensitivity − [1 − Specificity]) B-US 88.6% (62/70) 46.6% (27/58) 69.5% (89/128) 66.7% (62/93) 77.1% (27/35) 35.2% PDI 94.3% (66/70) 77.6% (45/58) ∗ 86.7% (111/128) ∗ 83.5% (66/79) ∗ 91.8% (45/49) 75.3% ∗ UE 92.8 % (65/70) 53.4% (31/58) ∗ † 75% (96/128) ∗ † 70.7% (65/92) † 86.1% (31/36) 46.3% †
B-US, B-mode ultrasound; NPV, negative predictive value; PDI, power Doppler imaging; PPV, positive predictive value; UE, ultrasound elastography.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
UE
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Interobserver Variability
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgment
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Layland M.K., Sessions D.G., Lenox J.: The influence of lymph node metastasis in the treatment of squamous cell carcinoma of the oral cavity, oropharynx, larynx, and hypopharynx: N0 versus N+. Laryngoscope 2005; 115: pp. 629-639.
2. Adoga A.A., Silas O.A., Nimkur T.L.: Open cervical lymph node biopsy for head and neck cancers: any benefit?. Head Neck Oncol 2009; 1: pp. 9.
3. Ross D.S.: Nonpalpable thyroid nodules: managing an epidemic. J Clin Endocrinol Metab 2002; 87: pp. 1938-1940.
4. Waki K, Murayama N, Matsumura T, et al. Investigation of strain ratio using ultrasound elastography technique. Presented at: First International Symposium on Information and Computer Elements; Kitakyushu, Japan; September 12–14, 2007.
5. Lyshchik A., Higashi T., Asato R., et. al.: Thyroid gland tumor diagnosis at US elastography. Radiology 2005; 237: pp. 202-211.
6. Cho N., Moon W.K., Park J.S., et. al.: Nonpalpable breast masses: evaluation by US elastography. Korean J Radiol 2008; 9: pp. 111-118.
7. Cochlin D.L., Ganatra R.H., Griffths D.F.: Elastography in the detection of prostatic cancer. Clin Radiol 2002; 57: pp. 1014-1020.
8. Giovannini M., Botelberge T., Bories E., et. al.: Endoscopic ultrasound elastography for evaluation of lymph nodes and pancreatic masses: a multicenter study. World J Gastroenterol 2009; 15: pp. 1587-1593.
9. Kirk G.D., Astemborski J., Mehta S.H., et. al.: Assessment of liver fibrosis by transient elastography in persons with hepatitis C virus infection or HIV-C hepatitis C virus coinfection. Clin Infect Dis 2009; 48: pp. 963-972.
10. Lyshchik A., Higashi T., Asato R., et. al.: Cervical lymph node metastasis: diagnosis at UE—initial experience. Radiology 2007; 243: pp. 258-267.
11. Frey H.: Real time elastography: a new ultrasound procedure for the reconstruction of tissue elasticity. J Radiol 2003; 43: pp. 850-855.
12. Furukawa M.K., Kubota A., Hanamura H., et. al.: Diagnosis of cervical lymph node metastasis of head and neck squamous cell carcinoma—usefulness of power Doppler ultrasonography and elastography. Medix 2007; pp. 20-23.
13. Kallel F., Ophir J.: Limits on the contrast of strain concentrations in elastography. Ultrasound Med Biol 1998; 24: pp. 1215-1219.
14. Vassallo P., Wernecke K., Roos N., et. al.: Differentiation of benign from malignant superficial lymphadenopathy: the role of high-resolution US. Radiology 1992; 183: pp. 215-220.
15. Wu C.-H., Hsu M.-M., Chang Y.-L., et. al.: Vascular pathology of malignant cervical lymphadenopathy: qualitative and quantitative assessment with power Doppler ultrasound. Cancer 1998; 83: pp. 1189-1196.
16. Loew J.M.: Lymph node diagnostic algorithm.Haber M.Mohr L.Helle M.Differential diagnosis on surgical pathology.2004.Qinghua University PressBeijing, China:pp. 883-886.
17. Byrne D.W.: Publishing your medical research paper: what they don’t teach in medical school.2002.Lippincott Williams & WilkinsBeijing, China 88–96
18. Qiu Y., Sridhar M., Tsou J.K., et. al.: Ultrasonic viscoelasticity imaging of nonpalpable breast tumors: preliminary results. Acad Radiol 2008; 15: pp. 1526-1533.
19. Chikui T., Yonetsu K., Nakamura T.: Multivariate feature analysis of sonographic findings of metastatic cervical lymph nodes: contribution of blood flow features revealed by power Doppler sonography for predicting metastasis. AJNR Am J Neuroadiol 2000; 21: pp. 561-567.
20. Alam F., Natio K., Horiguchi J., et. al.: Accuracy of sonographic elastography in the differential diagnosis of enlarged cervical lymph nodes: comparison with conventional B-mode sonography. AJR Am J Roentgenol 2008; 191: pp. 604-610.