
Rationale and Objectives
To determine the impact of additional coronary calcium scoring on total effective radiation dose and diagnostic accuracy of low-dose computed tomography coronary angiography (CTCA) with prospective electrocardiogram (ECG) triggering.
Materials and Methods
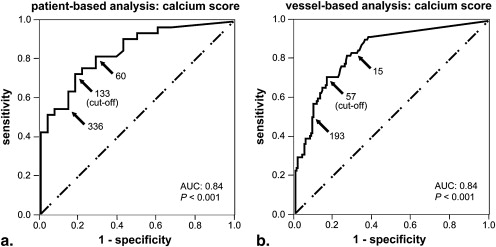
Sixty-one consecutive patients underwent 64-slice CTCA using prospective ECG triggering, calcium scoring, and invasive quantitative coronary angiography, the latter served as standard of reference. Diagnostic accuracy was calculated for CTCA, calcium scoring, and for the combination of both. Receiver operator characteristic analyses were performed to determine cutoffs for prediction of significant coronary artery stenoses.
Results
Mean effective radiation dose was 2.1 ± 0.7 mSv (range, 1.0–3.3 mSv) for CTCA and 1.1 ± 0.1 mSv (range, 0.9–1.4 mSv) for calcium scoring. Per-patient sensitivity, specificity, positive predictive value, and negative predictive value were 100%, 85.7%, 89.2%, and 100% for CTCA, and 72.7%, 82.1%, 82.8%, and 71.9% for calcium scoring. Adding calcium-scoring with a cutoff at 133 in patients aged >50.7 years with nondiagnostic CTCA improved the respective values of diagnostic accuracy of the entire study population to 100%, 96.4%, 97.1%, and 100%; the added value of calcium scoring was confined to only three patients (5%), who were reclassified from false positive to true negative.
Conclusion
Specificity and PPV of low-dose CTCA may be further improved by combining it with coronary calcium scoring. However, only a fraction of patient may benefit, whereas exposing the entire population to more than 50% increase in effective radiation dose.
Computed tomography coronary angiography (CTCA) with prospective electrocardiogram (ECG) triggering has recently been introduced and shown to offer a tremendous reduction of radiation dose compared to retrospective ECG-gating . Hence, a widespread clinical acceptance of noninvasive imaging of the coronary arteries with CTCA may now be envisioned. In selected patient populations with low heart rates, initial reports have demonstrated a high diagnostic accuracy of low dose CTCA with prospective ECG triggering compared to the current reference standard quantitative coronary angiography (QCA) , similar to the diagnostic accuracy achieved by retrospective ECG-gating technique .
However, the occurrence of artefacts leading to nondiagnostic image quality has been described . When artefacts render CTCA image quality nondiagnostic, patient examinations in clinical routine should be considered as positive and patients should be referred to further clinical work-up (ie, proof of stress-induced ischemia, invasive coronary angiography). Therefore, depending on the occurrence rate of nondiagnostic image quality, a considerable number of patients will unnecessarily undergo invasive coronary angiography, because of false-positive CTCA findings.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Patient Demographics
Number of patients 61 Age in years (mean ± SD, range) 61 ± 11, 30–85 Female gender ( n ) 24 Male gender ( n ) 37 Body mass index in kg/m 2 (mean ± SD, range) 27 ± 5, 19–45 Heart rate in bpm (mean ± SD, range) 56 ± 7, 36–70 Coronary risk factors ( n ) Smokers 28 Hypertension 36 Diabetes 4 Positive family history 22 Dyslipidemia 28 Calcium score (mean ± SD, range) 481 ± 885, 0–5477 Calcium score percentiles ( n ) <25th percentile 17 25–50th percentile 8 50–75th percentile 10 75–90th percentile 8 >90th percentile 18
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Diagnostic Accuracy of CTCA, Calcium Scoring, and of the Combination of Both
Sensitivity Specificity PPV NPV Patient-based CTCA 100% (33/33; NA) 85.7% (24/28; 67.3–95.9) 89.2% (33/37; 74.6–96.9) 100% (24/24; NA) Calcium score 72.7% (24/33; 54.5–86.7) 82.1% (23/28; 63.1–93.4) 82.8% (24/29; 64.2–94.2) 71.9% (23/32; 53.3–86.3) CTCA plus calcium score: 93.9% (31/33; 79.8–99.3) 96.4% (27/28; 81.6–99.9) 96.9% (31/32; 83.8–99.9) 93.1% (27/29; 77.2–99.2) CTCA plus calcium score, patients age >50.7 years: 100% (33/33; NA) 96.4% (27/28; 81.7–99.9) 97.1% (33/34; 84.7–99.9) 100% (27/27; NA) Vessel-based CTCA: computed tomography coronary angiography; NA: not available. 93.1% (67/72; 84.5–97.7) 85.5% (147/172; 79.3–90.4) 72.8% (67/92; 62.6–81.6) 96.7% (147/152; 92.5–98.9) Calcium score 70.8% (51/72; 58.9–80.9) 83.7% (144/172; 77.3–88.9) 64.6% (51/79; 53.0–75.0) 87.3% (144/165; 81.2–91.6) CTCA plus calcium score combined 93.1% (67/72; 84.5–97.7) 92.4% (159/172; 87.4–95.9) 83.8% (67/80; 73.8–91.1) 96.9% (159/164; 93.0–99.0) CTCA plus calcium score, patients age >68.8 years 93.1% (67/72; 84.5–97.7) 86.6% (149/172; 80.6–91.3) 74.4% (67/90; 64.2–83.1) 96.8% (149/154; 92.6–98.9)
CTCA: computed tomography coronary angiography.
Numbers in parenthesis correspond to the absolute values and the 95% confidence interval. PPV: positive predictive value. NPV: negative predictive value. NA: not available.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Hsieh J., Londt J., Vass M., et. al.: Step-and-shoot data acquisition and reconstruction for cardiac x-ray computed tomography. Med Phys 2006; 33: pp. 4236-4248.
2. Husmann L., Valenta I., Gaemperli O., et. al.: Feasibility of low-dose coronary CT angiography: first experience with prospective ECG-gating. Eur Heart J 2008; 29: pp. 191-197.
3. Earls J.P., Berman E.L., Urban B.A., et. al.: Prospectively gated transverse coronary CT angiography versus retrospectively gated helical technique: improved image quality and reduced radiation dose. Radiology 2008; 246: pp. 742-753.
4. Shuman W.P., Branch K.R., May J.M., et. al.: Prospective versus retrospective ECG gating for 64-detector CT of the coronary arteries: comparison of image quality and patient radiation dose. Radiology 2008; 248: pp. 431-437.
5. Hirai N., Horiguchi J., Fujioka C., et. al.: Prospective versus retrospective ECG-gated 64-detector coronary CT angiography: assessment of image quality, stenosis, and radiation dose. Radiology 2008; 248: pp. 424-430.
6. Herzog B.A., Husmann L., Valenta I., et. al.: Determinants of vessel contrast in BMI-adapted low dose CT coronary angiography with prospective ECG-triggering. Int J Cardiovasc Imaging 2009;
7. Scheffel H., Alkadhi H., Leschka S., et. al.: Low-dose CT coronary angiography in the step-and-shoot mode: diagnostic performance. Heart 2008; 94: pp. 1132-1137.
8. Maruyama T., Takada M., Hasuike T., et. al.: Radiation dose reduction and coronary assessability of prospective electrocardiogram-gated computed tomography coronary angiography: comparison with retrospective electrocardiogram-gated helical scan. J Am Coll Cardiol 2008; 52: pp. 1450-1455.
9. Herzog B.A., Husmann L., Burkhard N., et. al.: Accuracy of low-dose computed tomography coronary angiography using prospective electrocardiogram-triggering: first clinical experience. Eur Heart J 2008; 29: pp. 3037-3042.
10. Husmann L., Schepis T., Scheffel H., et. al.: Comparison of diagnostic accuracy of 64-slice computed tomography coronary angiography in patients with low, intermediate, and high cardiovascular risk. Acad Radiol 2008; 15: pp. 452-461.
11. Leber A.W., Knez A., Mukherjee R., et. al.: Usefulness of calcium scoring using electron beam computed tomography and noninvasive coronary angiography in patients with suspected coronary artery disease. Am J Cardiol 2001; 88: pp. 219-223.
12. Pundziute G., Schuijf J.D., Jukema J.W., et. al.: Impact of coronary calcium score on diagnostic accuracy of multislice computed tomography coronary angiography for detection of coronary artery disease. J Nucl Cardiol 2007; 14: pp. 36-43.
13. Leschka S., Scheffel H., Desbiolles L., et. al.: Combining dual-source computed tomography coronary angiography and calcium scoring: added value for the assessment of coronary artery disease. Heart 2008; 94: pp. 1154-1161.
14. Lau G.T., Ridley L.J., Schieb M.C., et. al.: Coronary artery stenoses: detection with calcium scoring, CT angiography, and both methods combined. Radiology 2005; 235: pp. 415-422.
15. Einstein A.J.: Radiation risk from coronary artery disease imaging: how do different diagnostic tests compare?. Heart 2008; 94: pp. 1519-1521.
16. Einstein A.J., Moser K.W., Thompson R.C., et. al.: Radiation dose to patients from cardiac diagnostic imaging. Circulation 2007; 116: pp. 1290-1305.
17. Austen W.G., Edwards J.E., Frye R.L., et. al.: A reporting system on patients evaluated for coronary artery disease. Report of the Ad Hoc Committee for Grading of Coronary Artery Disease, Council on Cardiovascular Surgery, American Heart Association. Circulation 1975; 51: pp. 5-40.
18. Garcia M.J., Lessick J., Hoffmann M.H.: Accuracy of 16-row multidetector computed tomography for the assessment of coronary artery stenosis. JAMA 2006; 296: pp. 403-411.
19. Schenker M.P., Dorbala S., Hong E.C., et. al.: Interrelation of coronary calcification, myocardial ischemia, and outcomes in patients with intermediate likelihood of coronary artery disease: a combined positron emission tomography/computed tomography study. Circulation 2008; 117: pp. 1693-1700.
20. Greenland P., Bonow R.O.: How low-risk is a coronary calcium score of zero? The importance of conditional probability. Circulation 2008; 117: pp. 1627-1629.
21. Rybicki F.J., Otero H.J., Steigner M.L., et. al.: Initial evaluation of coronary images from 320-detector row computed tomography. Int J Cardiovasc Imaging 2008; 24: pp. 535-546.
22. van Werkhoven J.M., Schuijf J.D., Gaemperli O., et. al.: Incremental prognostic value of multi-slice computed tomography coronary angiography over coronary artery calcium scoring in patients with suspected coronary artery disease. Eur Heart J 2009 June 29; [Epub ahead of print]