
Rationale and Objectives
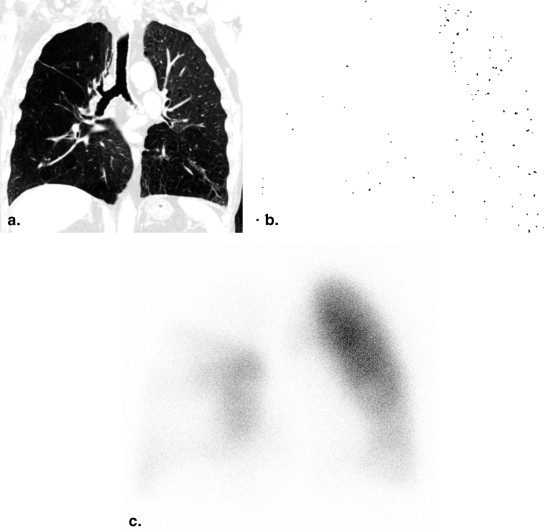
Cross-sectional area <5 mm 2 (CSA<5) is a computed tomography (CT) metric that has been used for the evaluation of pulmonary vessel alterations and perfusion. CSA<5 is calculated from three axial slices; thus, whether CSA<5 represents the small pulmonary vessel alterations in the whole lung remains unclear. The purpose of this study was to compare the measurements of CSA<5 using three axial slices and coronal reconstructed slices in the relationship between the measured CSA<5 and pulmonary perfusion measured using lung perfusion scintigraphy.
Materials and Methods
This study comprised 28 subjects who underwent both noncontrast CT and lung perfusion scintigraphy. The present study measured CSA<5 using both three axial CT images and coronal reconstruction images and then obtained the percentage of the CSA in right lung to that in whole lung (R/W-CSA<5). Using anteroposterior and posteroanterior projections on technetium-99m macroaggregated albumin (MAA) lung perfusion scintigraphy, we obtained right and total lung counts and calculated the percentage of the right to whole lung counts (R/W-MAA). The correlations of the R/W-CSA<5 calculated using three axial slices (R/W-CSA Ax <5) and coronal reconstructed slices (R/W-CSA COR <5) with R/W-MAA were evaluated using Spearman rank correlation analysis.
Results
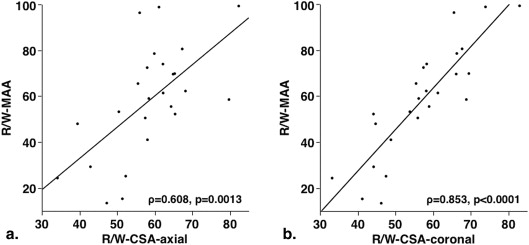
Both R/W-CSA Ax <5 and R/W-CSA COR <5 were significantly correlated with R/W-MAA; however, the correlation coefficient with R/W-CSA COR <5 (ρ = 0.842, P < .0001) was greater than that with R/W-CSA Ax <5 (ρ = 0.631, P = .0004).
Conclusions
Coronal reconstruction images appear suitable for quantitative measurement of CSA of small pulmonary vessels.
To understand the pathophysiologic manifestations of a variety of lung diseases, it is necessary to evaluate morphologic alterations in the pulmonary vasculature. Morphologic vascular alterations are linked with both pulmonary ventilation and perfusion. For instance, morphologic vascular alteration is one of the characteristic histologic features of chronic obstructive pulmonary disease (COPD) , while vascular alteration is related to both airflow limitation and decreased pulmonary perfusion, which can lead to pulmonary hypertension .
Pulmonary vascular alterations are difficult to evaluate quantitatively in vivo. Therefore, several investigations have been conducted on various lung diseases proposing the use of computed tomography (CT) for the quantitative evaluation of morphologic vascular alterations of the cross-sectional area (CSA) of small pulmonary vessels . In fact, significant correlations have been reported between the CSA of small pulmonary vessels and both pulmonary perfusion and degree of pulmonary hypertension .
Get Radiology Tree app to read full this article<
Materials and methods
Subjects
Get Radiology Tree app to read full this article<
CT Protocol
Get Radiology Tree app to read full this article<
CT Measurement of Small Pulmonary Vessels
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Pulmonary Perfusion Scintigraphy
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
CT Measurements and Scintigraphy Measurements
%CSA Ax <5 (%) 0.64 ± 0.21 %CSA COR <5 (%) 0.58 ± 0.22 R/W-CSA Ax <5 (%) 59.0 ± 10.7 R/W-CSA COR <5 (%) 57.5 ± 11.3 R/W-CSA COR-DA <5 (%) 57.5 ± 13.2 R/W-CSA COR-TR <5 (%) 55.4 ± 11.5 R/W-CSA COR-AA <5 (%) 60.8 ± 14.4 R/W-MAA (%) 59.6 ± 24.4
CSA<5, the cross-sectional area of pulmonary vessels <5 mm 2 ; MAA, macroaggregated albumin.
Table 2
Correlations Between R/W-MAA and R/W-CSA
ρ_P_ R/W-CSA Ax <5 (%) 0.631 .0004 R/W-CSA COR <5 (%) 0.842 <.0001 R/W-CSA COR-DA <5 (%) 0.727 <.0001 R/W-CSA COR-TR <5 (%) 0.764 <.0001 R/W-CSA COR-AA <5 (%) 0.897 <.0001
CSA<5, the cross-sectional area of pulmonary vessels <5 mm 2 ; MAA, macroaggregated albumin.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Hale K.A., Niewoehner D.E., Cosio M.G.: Morphologic changes in the muscular pulmonary arteries: relationship to cigarette smoking, airway disease, and emphysema. Am Rev Respir Dis 1980; 122: pp. 273-278.
2. Barbera J.A., Riverola A., Roca J., et. al.: Pulmonary vascular abnormalities and ventilation perfusion relationships in mild chronic obstructive pulmonary disease. Am J Respir Crit Care Med 1994; 149: pp. 423-429.
3. Kubo K., Ge R.L., Koizumi T., et. al.: Pulmonary artery remodeling modifies pulmonary hypertension during exercise in severe emphysema. Respir Physiol 2000; 120: pp. 71-79. Cottin V, Nunes H, Brillet PY, et al. Combined pulmonary fibrosis and emphysema: a distinct under recognised entity. Eur Respir J 2005;26:586-593
4. Matsuoka S., Washko G.R., Dransfield M.T., et. al.: Quantitative CT Measurement of cross-sectional area of small pulmonary vessel in COPD: correlations with emphysema and airflow limitation. Acad Radiol 2010; 17: pp. 93-99.
5. Matsuoka S., Washko G.R., Yamashiro T., et. al.: Pulmonary hypertension and CT measurement of small pulmonary vessels in severe emphysema. Am J Respir Crit Care Med 2010; 181: pp. 218-225.
6. Matsuoka S., Yamashiro T., Diaz A., et. al.: The relationship between small pulmonary vascular alteration and aortic atherosclerosis in chronic obstructive pulmonary disease: quantitative CT analysis. Acad Radiol 2011; 18: pp. 40-46.
7. Uejima I., Matsuoka S., Yamashiro T., et. al.: Quantitative computed tomographic measurement of a cross-sectional area of a small pulmonary vessel in nonsmokers without airflow limitation. Jpn J Radiol 2011; 29: pp. 251-255.
8. Ando K., Tobino K., Kurihara M., et. al.: Quantitative CT analysis of small pulmonary vessels in lymphangioleiomyomatosis. Eur J Radiol 2012; 81: pp. 3925-3930.
9. Matsuura Y., Kawata N., Yanagawa N., et. al.: Quantitative assessment of cross-sectional area of small pulmonary vessels in patients with COPD using inspiratory and expiratory MDCT. Eur J Radiol 2013; 82: pp. 1804-1810.
10. Ando K., Sekiya M., Tobino K., et. al.: Relationship between quantitative CT metrics and pulmonary function in combined pulmonary fibrosis and emphysema. Lung 2013; 191: pp. 585-591.
11. Matsuoka S., Yamashiro T., Matsushita S., et. al.: Relationship between quantitative CT of pulmonary small vessels and pulmonary perfusion. AJR Am J Roentgenol 2014; 202: pp. 719-724.
12. DeMeester T.R., Van Heertum R.L., Karas J.R., et. al.: Preoperative evaluation with differential pulmonary function. Ann Thorac Surg 1974; 18: pp. 61-71.
13. Boysen P.G., Block A.J., Olsen G.N., et. al.: Prospective evaluation for pneumonectomy using the 99mtechnetium quantitative perfusion lung scan. Chest 1977; 72: pp. 422-425.
14. Fleischmann D., Rubin G.D., Paik D.S., et. al.: Stair-step artifacts with single versus multiple detector-row helical CT. Radiology 2000; 216: pp. 185-196.
15. Park K.J., Bergin C.J., Clausen J.L.: Quantitation of emphysema with three-dimensional CT densitometry: comparison with two-dimensional analysis, visual emphysema scores, and pulmonary function test results. Radiology 1999; 211: pp. 541-547.
16. Kauczor H.U., Heussel C.P., Fischer B., et. al.: Assessment of lung volumes using helical CT at inspiration and expiration: comparison with pulmonary function tests. AJR Am J Roentgenol 1998; 171: pp. 1091-1095.
17. Estépar R.S., Kinney G.L., Black-Shinn J.L., et. al.: Computed tomographic measures of pulmonary vascular morphology in smokers and their clinical implications. Am J Respir Crit Care Med 2013; 188: pp. 231-239.