
Purpose
Medicare requires documented teaching physician involvement (attestation) in trainee-generated radiology reports. Automated attestation statement insertion in reports expedites the process but does not comply with requirements for active attestation. We evaluated an informatics-enabled quality improvement (QI) intervention to improve health record documentation requirements for active attestation.
Materials and Methods
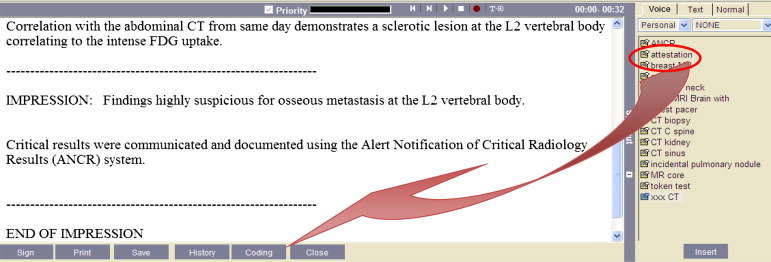
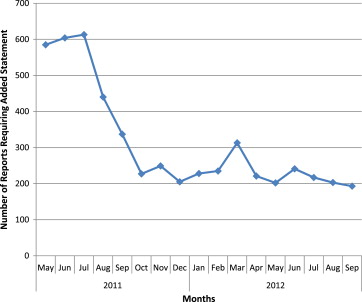
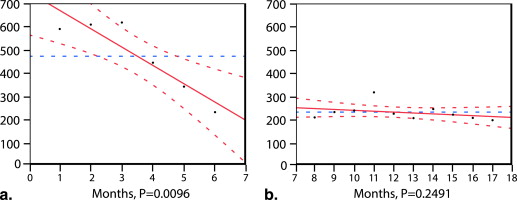
Institutional review board approval was not needed for this QI project performed in a 776-bed tertiary/quaternary teaching hospital. The intervention consisted of (1) policy requiring staff radiologists to actively attest to trainee-generated reports by personally activating a “macro” in the reporting system and (2) a semiautomated process to detect reports missing attestation; radiologists received daily e-mail reminders until the attestation statement was inserted. A random sample of 600 of 123,561 trainee-generated radiology reports created 17 months after the intervention (May 2011) was manually reviewed to determine attestation policy adherence. The number of attestation statements added in response to reminders throughout the entire study period was also evaluated. Trend analysis of the number of report addenda containing solely the attestation statement (proxy for missing initial attestation) was performed.
Results
Of 600 reports, 594 (99%) contained the attestation statement. Monthly attestations in response to email notifications decreased from 585 to 227 by the sixth month, a 2.6-fold reduction ( P < .01). No significant trend was observed the following year, indicating a sustained effect.
Conclusion
Informatics-enabled QI techniques resulted in 99% adherence to our teaching physician attestation policy with sustained results. Similar approaches may help improve adherence to other mandated performance measures in radiology reports.
Radiologists in both academic and private practice settings must document specific content in radiology reports to meet an increasing number of quality measures , safety goals , or compliance requirements . Reporting templates created within speech recognition software or structured reporting applications can remind and encourage radiologists to document specific content in their reports. However, it is unclear whether such technology interventions alone can uniformly guarantee capture of needed content in radiology reports. Moreover, such approaches will require all radiologists to use report templates [e.g., the structured reporting templates of the Radiological Society of North America ] for every report they create, which may be challenging in the short term.
As an example, Medicare Part B requires documentation of teaching physician involvement (attestation) in trainee-generated radiology reports . Institutions have taken several approaches to address this requirement; some academic radiology departments automatically add the attestation statement at the end of all trainee-generated reports, others allow the trainee to enter the attestation statement, and some require staff radiologists to attest . The interpretation of the relevant Centers for Medicare and Medicaid Services (CMS) teaching physician attestation policy by our institution’s compliance officer requires staff radiologists to actively attest (rather than using an automated attestation process) by entering an attestation statement at the time of final signature in each radiology report created by a trainee. Trainee-entered attestation statements were deemed to create a quality and compliance risk, as the report would contain the attestation statement even before an attending radiologist signature.
Get Radiology Tree app to read full this article<
Materials and methods
Setting
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Preintervention Trainee-Generated Report Approval Workflow
Get Radiology Tree app to read full this article<
Intervention
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Study Period
Get Radiology Tree app to read full this article<
Data Collection
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Centers for Medicare & Medicaid Services. Overview Physician Quality Reporting Initiative. Available from: http://www.cms.hhs.gov/pqri/ . Accessed March 24, 2010.
2. Berlin L.: Communicating findings of radiologic examinations: whither goest the radiologist’s duty?. AJR Am J Roentgenol 2002; 178: pp. 809-815.
3. 2013 National Patient Safety Goals. Available from: http://www.jointcommission.org/hap_2013_npsg/default.aspx . Accessed January 21, 2013.
4. Centers for Medicare and Medicaid Services . Pub 100-04 Medicare claims processing: transmittal 811. Available from: http://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/downloads/R811CP.pdf . Accessed November 14, 2012.
5. Radiological Society of North America. Radiology Reporting Initiative. Available from: https://www.rsna.org/Reporting_Initiative.aspx . Accessed January 21, 2013.
6. Hunter T.B., Krupinski E.: Faculty attestation statements for resident-generated radiology reports. J Am Coll Radiol 2011; 8: pp. 727-730.
7. Andriole K.P., Prevedello L.M., Dufault A., et. al.: Augmenting the impact of technology adoption with financial incentive to improve radiology report signature times. J Am Coll Radiol 2010; 7: pp. 198-204.
8. Anthony S.G., Prevedello L.M., Damiano M.M., et. al.: Impact of a 4-year quality improvement initiative to improve communication of critical imaging test results. Radiology 2011; 259: pp. 802-807.
9. Mendiratta-Lala M., Eisenberg R.L., Steele J.R., et. al.: Quality initiatives: measuring and managing the procedural competency of radiologists. Radiographics 2011; 31: pp. 1477-1488.
10. Gershanik E.F., Lacson R., Khorasani R.: Critical finding capture in the impression section of radiology reports. AMIA Annu Symp Proc 2011; 2011: pp. 465-469.
11. Lacson R., Andriole K.P., Prevedello L.M., et. al.: Information from Searching Content with an Ontology-Utilizing Toolkit (iSCOUT). J Digit Imaging 2012; 25: pp. 512-519.
12. Rubin D., Wang D., Chambers D.A., et. al.: Natural language processing for lines and devices in portable chest x-rays. AMIA Annu Symp Proc 2010; 2010: pp. 692-696.
13. Lacson R., Sugarbaker N., Prevedello L.M., et. al.: Retrieval of radiology reports citing critical findings with disease-specific customization. Open Med Inform J 2012; 6: pp. 28-35.
14. Garla V., Lo Re V., Dorey-Stein Z., et. al.: The Yale cTAKES extensions for document classification: architecture and application. J Am Med Inform Assoc 2011; 18: pp. 614-620.