
Rationale and Objectives
A picture archiving and communication system (PACS)–integrated ultrasound-guided (USG) breast intervention simulation exercise was designed for radiology residency education. The purpose of this study was to describe the initial experience and determine if resident understanding of the American College of Radiology (ACR) practice guideline for the performance of USG percutaneous breast interventional procedures and procedural confidence is improved with the implementation of this simulation exercise.
Materials and Methods
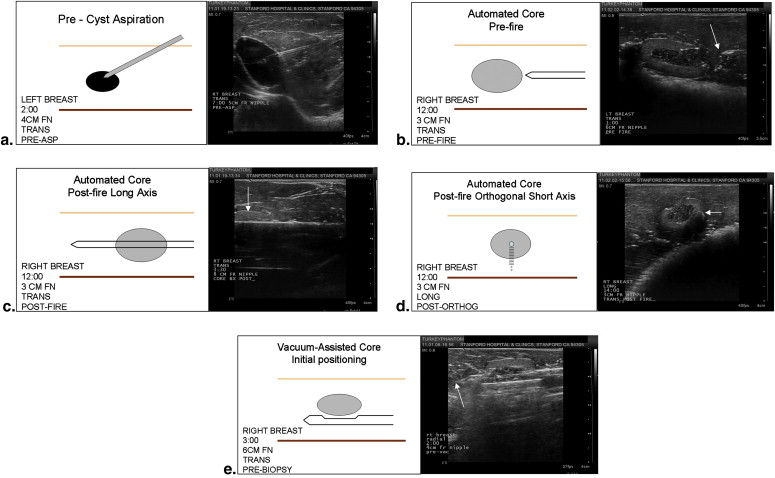
Radiology residents ( n = 11) volunteered to perform percutaneous USG cyst aspiration, 14-gauge automated core biopsy, and 10-gauge vacuum core biopsy on turkey breast phantoms, with an emphasis on capturing ultrasound images demonstrating appropriate documentation of the procedure and image annotation according to the ACR practice guideline for USG percutaneous interventions. The images were transmitted to the PACS for subsequent attending radiologist review. Survey responses regarding procedural confidence and knowledge of the ACR practice guideline were compared between residents with and without the simulator experience.
Results
Residents with simulation exercise experience showed statistically significant increases in confidence performing USG core biopsies, operating biopsy devices and ultrasound equipment, and knowledge of appropriate needle positioning and image annotation and documentation according to the ACR practice guideline. The increased confidence seen in performing USG cyst aspiration barely missed statistical significance ( P = .056), likely because of residents’ baseline familiarity with the procedure.
Conclusions
A PACS-integrated USG breast intervention simulation exercise increases residents’ procedural confidence and understanding of the ACR practice guideline for the performance of USG percutaneous breast interventional procedures.
Ultrasound-guided (USG) percutaneous breast interventions are important diagnostic and therapeutic procedures performed by radiologists and offer many advantages, including real-time imaging, a lack of ionizing radiation, and increased patient tolerance for supine positioning without breast compression. Many large-scale studies have validated the diagnostic accuracy of USG percutaneous core needle biopsy compared to surgical excision . Furthermore, the performance of USG percutaneous breast interventions has been associated with a decrease in the number of surgical procedures , improved cosmesis , and lower health care costs . In addition to these diagnostic procedures, cyst aspirations are often performed for therapeutic reasons, including alleviation of pain associated with benign breast cysts.
In October 2009, the American College of Radiology (ACR) revised its practice guideline for the performance of USG percutaneous breast interventional procedures to assist practitioners in achieving the objective of appropriate radiologic care for patients . This guideline may also serve as an educational outline to define core competencies for radiology residents.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Survey Results From Residents ( n = 13) Who Did Not Participate in the USG Breast Intervention Simulation Exercise
Survey Item 1 (Poor) 2 3 (Average) 4 5 (Good) Mean Confidence in ability to perform vacuum core biopsy 6 (46%) 3 (23%) 2 (15%) 2 (15%) 0 (0%) 2 Confidence in ability to perform cyst aspiration 2 (15%) 0 (0%) 5 (38%) 4 (31%) 2 (15%) 3.3 Confidence in ability to perform automated core biopsy 3 (23%) 5 (38%) 1 (8%) 4 (31%) 0 (0%) 2.5 Understanding of needle positioning 2 (15%) 3 (23%) 3 (23%) 4 (31%) 1 (8%) 2.9 Comfort level operating biopsy devices 2 (15%) 6 (46%) 2 (15%) 3 (23%) 0 (0%) 2.5 Comfort level operating ultrasound equipment 2 (15%) 3 (23%) 3 (23%) 4 (31%) 1 (8%) 2.9 Understanding of ACR image documentation and annotation 5 (38%) 3 (23%) 4 (31%) 1 (8%) 0 (0%) 2.1
Percentages may not total 100% because of rounding.
ACR, American College of Radiology; USG, ultrasound-guided.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Survey Results From Residents ( n = 11) Who Participated in the USG Breast Intervention Simulation Exercise
Survey Item 1 (Poor) 2 3 (Average) 4 5 (Good) Mean_P_ Confidence in ability to perform vacuum core biopsy 0 (0%) 1 (9%) 7 (64%) 1 (9%) 2 (18%) 3.4 .012 Confidence in ability to perform cyst aspiration 0 (0%) 0 (0%) 0 (0%) 9 (82%) 2 (18%) 4.2 .056 Confidence in ability to perform automated core biopsy 0 (0%) 1 (9%) 4 (36%) 5 (45%) 1 (9%) 3.6 .039 Understanding of needle positioning 0 (0%) 0 (0%) 2 (18%) 5 (45%) 4 (36%) 4.2 .017 Comfort level operating biopsy devices 0 (0%) 0 (0%) 4 (36%) 4 (36%) 3 (27%) 3.9 .004 Comfort level operating ultrasound equipment 0 (0%) 0 (0%) 3 (27%) 4 (36%) 4 (36%) 4.1 .030 Understanding of ACR image documentation and annotation 0 (0%) 2 (18%) 0 (0%) 5 (45%) 4 (36%) 4 .001
Percentages may not total 100% because of rounding. P values < .05 were considered statistically significant.
ACR, American College of Radiology; USG, ultrasound-guided.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
References
1. Parker S.H., Jobe W.E., Dennis M.A., et. al.: US-guided automated large-core breast biopsy. Radiology 1993; 187: pp. 507-511.
2. Parker S.H., Burbank F., Jackman R.J.: Percutaneous large-core breast biopsy: a multi-institutional study. Radiology 1994; 193: pp. 359-364.
3. Meyer J.E., Smith D.N., Lester S.C., et. al.: Large-core needle biopsy of nonpalpable breast lesions. JAMA 1999; 281: pp. 1638-1641.
4. Verkooijen H.M., Peeters P.H., Buskens E., et. al.: Diagnostic accuracy of large-core needle biopsy for nonpalpable breast disease: a meta-analysis. Br J Cancer 2000; 82: pp. 1017-1021.
5. Fajardo L.L., Pisano E.D., Caudry D.J., et. al.: Radiologist Investigators of the Radiologic Diagnostic Oncology Group V Study. Stereotactic and sonographic large-core biopsy of nonpalpable breast lesions: results of the Radiologic Diagnostic Oncology Group V study. Acad Radiol 2004; 11: pp. 293-308.
6. Youk J., Kim E.K., Kim M.J., et. al.: Sonographically guided 14-gauge core needle biopsy of breast masses: a review of 2,420 cases with long-term follow-up. AJR Am J Roentgenol 2008; 190: pp. 202-207.
7. Smith D.N., Christian R.L., Meyer J.E.: Large-core needle biopsy of non-palpable breast cancers: the impact on subsequent surgical excisions. Arch Surg 1997; 132: pp. 256-259.
8. Liberman L., LaTrenta L.R., Dershaw D.D., et. al.: Impact of core biopsy on the surgical management of impalpable breast cancer. AJR Am J Roentgenol 1997; 168: pp. 495-499.
9. Wang W.J., Wang Q., Cai Q.P., et. al.: Ultrasonographically guided vacuum-assisted excision for multiple breast masses: non-randomized comparison with conventional open excision. J Surg Oncol 2009; 100: pp. 675-680.
10. Liberman L., Feng T.L., Dershaw D.D., et. al.: Ultrasound-guided core breast biopsy: Utility and cost-effectiveness. Radiology 1998; 208: pp. 717-723.
11. American College of Radiology. ACR practice guideline for the performance of ultrasound-guided percutaneous breast interventional procedures. Available at: http://www.acr.org/secondarymainmenucategories/quality_safety/guidelines/breast/us_guided_breast.aspx . Accessed March 30 2011.
12. Crofton M., Nicholson R.A.: Training phantom for ultrasound guided biopsy. Br J Radiol 1997; 70: pp. 192-194.
13. Harvey J.A., Moran R.E., Hamer M.M., et. al.: Evaluation of a turkey-breast phantom for teaching freehand US-guided core-needle breast biopsy. Acad Radiol 1997; 4: pp. 565-569.
14. Morehouse H., Thaker H.P., Persaud C.: Addition of Metamucil to gelatin for a realistic breast biopsy phantom. J Ultrasound Med 2007; 26: pp. 1123-1126.
15. Larrison M., Dibona A., Hogg D.E.: Low-cost phantom for stereotactic breast biopsy training. AJR Am J Roentgenol 2006; 187: pp. 972-974.
16. Bassett L.W., Monsees B.S., Wang L., et. al.: Survey of radiology residents: breast imaging training and attitudes. Radiology 2003; 227: pp. 862-869.
17. Hassard M.K., McCurdy L.I., Williams J.C., et. al.: Training module to teach ultrasound-guided breast biopsy skills to residents improves accuracy. Can Assoc Radiol J 2003; 54: pp. 155-159.
18. Baker J.A., Soo M.S.: Breast US: assessment of technical quality and image interpretation. Radiology 2002; 223: pp. 229-238.
19. Zou L., King A., Soman S., et. al.: Medical students’ preferences in radiology education: a comparison between the Socratic and didactic methods utilizing PowerPoint features in radiology education. Acad Radiol 2011; 18: pp. 253-256.
20. Phal P.M., Brooks D.M., Wolfe R.: Sonographically guided biopsy of focal lesions: a comparison of freehand and probe-guided techniques using a phantom. AJR Am J Roentgenol 2005; 184: pp. 1652-1656.
21. Bluvol N., Kornecki A., Shaikh A., et. al.: Freehand versus guided breast biopsy: comparison of accuracy, needle motion, and biopsy time in a tissue model. AJR Am J Roentgenol 2009; 192: pp. 1720-1725.
22. Mainiero M.B., Gareen I.F., Bird C.E., et. al.: Preferential use of sonographically guided biopsy to minimize patient discomfort and procedure time in a percutaneous image-guided breast biopsy program. J Ultrasound Med 2002; 21: pp. 1221-1226.