
Rationale and Objectives
This study aimed to develop and validate a method for measuring the depth of tumor invasion (DoI) using magnetic resonance imaging (MRI) and to investigate the diagnostic performance of the measured DoI for stratifying tumor (T) classification in patients with distal bile duct cancer according to the new American Joint Committee on Cancer staging system.
Materials and Methods
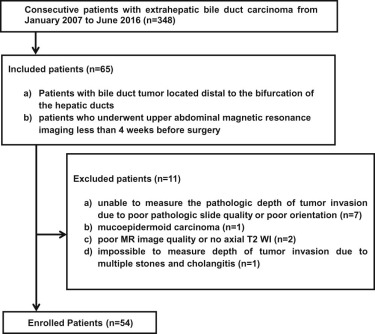
Fifty-four patients (30 men and 24 women; age range, 43–81 years) with distal bile duct cancer were enrolled. A study coordinator first developed a “provisional method” for measuring DoI on T2-weighted MRI. Subsequently, after compensating for defects, the “improved method” was developed. Two reviewers independently measured DoI and assessed its correlations with the histopathologic reference standard using intraclass correlation coefficient (ICC). The study population was grouped according to the DoI for T classification based on the new staging system for evaluation of diagnostic predictive values.
Results
The ICC values between the radiologic and the histopathologic DoI were calculated. Using the “improved method,” the ICC for the coordinator’s DoI was very good (ICC, 0.885), which was a significantly higher value than that obtained using the “provisional method” (ICC, 0.501, P = .00000); and for two reviewers’ DoIs, the ICC values were good (ICC, 0.752 and 0.784, respectively). The overall accuracy of MRI for stratifying bile duct tumors using DoI was 87.0% and 85.2%, respectively.
Conclusions
This newly developed method reliably measured DoI on T2-weighted MRI and can be used for preoperative T classification of patients with distal bile duct cancer according to the new staging system.
Introduction
Bile duct carcinoma is an uncommon neoplasm that accounts for 3% of all gastrointestinal cancers worldwide , and distal bile duct cancer accounts for 20%–30% of all bile duct carcinomas . Despite advances in surgical techniques and the introduction of developed oncologic modalities, the overall prognosis of bile duct cancer remains poor. As for other gastrointestinal tumors, tumor (T) classification is a major prognostic indicator in bile duct cancer. However, several studies have reported problems with T-staging using the seventh or former editions of the American Joint Committee on Cancer (AJCC) staging system . According to these systems, the T1 and T2 stages of distal bile duct cancer are distinguished on the basis of the extent of tumor within or beyond the bile duct wall, and T2 and T3 stages are distinguished on the basis of the presence or absence of adjacent organ invasion, including invasion of the gallbladder, duodenum, and pancreas . However, it has been noted that the staging system using descriptive extent of tumor invasion is associated with certain problems from both histopathologic and clinical aspects. For these reasons, several studies have suggested an alternative T-staging system using the depth of tumor invasion (DoI) to overcome the problems of the old T classification system , and the primary tumor staging of distal bile duct cancer in the eighth AJCC staging system was changed accordingly . In the new staging system, the definitions of T1, T2, and T3 have been revised based on measured DoI, which is better for predicting patient outcome and allows more reproducible measurements.
Magnetic resonance imaging (MRI) and multidetector computed tomography are useful modalities for the preoperative evaluation of bile duct cancer in terms of diagnosis, characterization, localization, and staging . For the diagnosis of bile duct cancer, information regarding the extent of the tumor and its resectability obtained with contrast-enhanced MRI and magnetic resonance (MR) cholangiography shows a diagnostic performance similar to information obtained using multidetector computed tomography and direct cholangiography . However, MRI is better than computed tomography for the visualization of intraductal lesions and the assessment of lateral extensions of extrahepatic bile duct cancer because of its superior contrast resolution and recent advances in MRI techniques. If the DoI of bile duct cancer can be accurately assessed using preoperative MRI, it might be used as a prognostic indicator.
Get Radiology Tree app to read full this article<
Materials and Methods
Get Radiology Tree app to read full this article<
Study Subjects
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Histopathologic Review
Get Radiology Tree app to read full this article<
MRI Techniques
Get Radiology Tree app to read full this article<
Image Analysis
Get Radiology Tree app to read full this article<
TABLE 1
Summary of Methods Proposed in the Current Study for the Measurement of Depth of Tumor Invasion (DoI) of Distal Bile Duct Cancer
 Open full size image
Open full size image
![Figure 2, Magnetic resonance ( a ) and microscopic (hematoxylin-eosin [H&E]) ( b ) images of the distal bile duct of a 75-year-old man with distal bile duct cancer. ( a ) The coronal T2-weighted image shows wall thickening of the distal bile duct with intact bile duct wall structure (arrowheads). The depth of tumor invasion (DoI) was defined as the maximal distance (double-headed arrow) between the innermost border of the bile duct wall and the outermost border of the tumor. The DoI measurements obtained by the two reviewers were 7.55 mm and 7.89 mm, respectively. ( b ) In tumors with flat or infiltrative patterns, the DoI was defined as the distance from the basal lamina or the surface of the tumor to the deepest invasive foci, and the histopathologic measurement of the DoI was 7.1 mm.](https://storage.googleapis.com/dl.dentistrykey.com/clinical/ValidationofFeasibilityofMagneticResonanceImagingfortheMeasurementofDepthofTumorInvasioninDistalBileDuctCancerAccordingtotheNewAmericanJointCommitteeonCancerStagingSystem/1_1s20S1076633217303021.jpg)

![Figure 4, Magnetic resonance ( a, b ) and microscopic (hematoxylin-eosin [H&E]) ( c ) images of the distal bile duct of a 73-year-old woman with distal bile duct cancer. ( a, b) The axial T2-weighted image shows eccentric wall thickening with an intraductal component (arrowheads) in the distal bile duct. The depth of tumor invasion (DoI) was defined as the maximal distance (double-headed arrow) between the imaginary line (dotted line on ( b )) connecting the two break points of the bile duct wall and the outermost border of the tumor. The DoI measurements obtained by the two reviewers were 7.53 mm and 6.99 mm, respectively. ( c ) In tumors with papillary or intraductal growth patterns, the DoI was defined as the distance from the basal lamina of the adjacent flat epithelium (and not from the top surface of the tumor) to the deepest invasive foci, and the histopathologic measurement of the DoI was 5.3 mm.](https://storage.googleapis.com/dl.dentistrykey.com/clinical/ValidationofFeasibilityofMagneticResonanceImagingfortheMeasurementofDepthofTumorInvasioninDistalBileDuctCancerAccordingtotheNewAmericanJointCommitteeonCancerStagingSystem/3_1s20S1076633217303021.jpg)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analyses
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
TABLE 2
Demographics and Clinicopathologic Characteristics of Study Subjects
Characteristics Datum ( n = 54) Age \* (y) 67.11 (43–81) Gender Male 30 (55.6) Female 24 (44.4) Surgery Conventional pancreaticoduodenectomy 2 (3.7) Pylorus-preserving pancreaticoduodenectomy 32 (59.3) Bile duct resection 20 (37.0) Histologic grade Well-differentiated 17 (31.5) Moderately differentiated 32 (59.3) Poorly differentiated 5 (9.3) Local tumor staging according to AJCC seventh edition T1 4 (7.4) T2 22 (40.7) T3 28 (51.9)
AJCC, American Joint Committee on Cancer.
Unless otherwise indicated, data are numbers of patients with percentages in parentheses.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 3
Magnetic Resonance Imaging and Histopathologic Features of Three Outlier Patients Obtained from a Bland-Altman Plot Showing the Agreement Between the Histopathologic DoI and Coordinator’s Measured DoI (95% Limits of Agreement)
Patient No. Location SI of Tumor on T2-weighted Image Main Pancreatic Dilatation with Abrupt Narrowing Measured DoI Using “Provisional Method” (mm) Histopathologic DoI (mm) Fig. No. 1 Intrapancreatic CBD Tumor SI indistinguishable from pancreas parenchymal SI Absent 5.00 20.0 Figure 6 2 Intrapancreatic CBD Tumor SI indistinguishable from pancreas parenchymal SI Present 4.79 19.0 Not shown 3 Intrapancreatic CBD Tumor SI indistinguishable from pancreas parenchymal SI Present 3.95 12.4 Figure 5
CBD, common bile duct; DoI, depth of tumor invasion; SI, signal intensity.
![Figure 5, Consecutive magnetic resonance ( a, b ) and microscopic (hematoxylin-eosin [H&E]) ( c ) images of the distal bile duct of a 68-year-old man with distal bile duct cancer. ( a ) The axial T2-weighted image that was obtained at the level of the suprapancreatic distal bile duct shows bile duct wall thickening (arrow) and dilatation of the main pancreatic duct (*). ( b ) The axial T2-weighted image that was obtained at the level of the intrapancreatic distal bile duct shows a bile duct tumor with a margin that is indistinguishable from the pancreatic parenchyma. The depth of tumor invasion (DoI) was defined as the maximal distance (double-headed arrow) between the tumor and the site of the main pancreatic duct obstruction. The radiologic DoI measurement that was made with the “provisional method” was 3.95 mm. With the “improved method,” the DoI measurements obtained by the two reviewers were 8.3 mm and 10.75 mm, respectively. ( c ) A photomicrograph showing a tumor with deep pancreatic invasion that caused abrupt narrowing of the main pancreatic duct and upstream duct dilatation (*). The histopathologic measurement of the DoI was 12.4 mm.](https://storage.googleapis.com/dl.dentistrykey.com/clinical/ValidationofFeasibilityofMagneticResonanceImagingfortheMeasurementofDepthofTumorInvasioninDistalBileDuctCancerAccordingtotheNewAmericanJointCommitteeonCancerStagingSystem/4_1s20S1076633217303021.jpg)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 4
Diagnostic Predictive Values of Magnetic Resonance Imaging (MRI) for T-staging Based on the New American Joint Committee on Cancer (AJCC) Staging System Using Depth of Tumor Invasion (DoI)
MRI Subclassification Based on the New AJCC Staging System Using DoI Histopathologic T stage Based on the New Staging System Using DoI Accuracy (%) Sensitivity (%) Specificity (%) T1 ( n = 29) T2 ( n = 21) T3 ( n = 4) Reviewer 1 T1 27 2 0 92.6 (50/54) 93.1 (27/29) 92 (23/25) T2 2 18 2 87.0 (47/54) 85.7 (18/21) 87.9 (29/33) T3 0 1 2 94.4 (51/54) 50 (2/4) 98 (49/50) Reviewer 2 T1 25 2 0 88.9 (48/54) 86.2 (25/29) 92 (23/25) T2 4 19 2 85.2 (46/54) 90.5 (19/21) 81.8 (27/33) T3 0 0 2 96.3 (52/54) 50 (2/4) 100 (50/50)
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
![Figure 6, Magnetic resonance (MR) ( a ) and microscopic (hematoxylin-eosin [H&E]) ( b ) images of the distal bile duct of a 54-year-old woman with distal bile duct cancer. ( a ) The axial T2-weighted image shows a bile duct tumor with a margin that is hardly distinguishable from the pancreatic parenchyma. The radiologic DoI measurement that was made with the “provisional method” was 5.0 mm. With the “improved method,” the DoI measurements obtained by the two reviewers were 5.3 mm and 5.8 mm, respectively. When the MR images were retrospectively reviewed with reference to the histopathologic results, the full thickness of the pancreas parenchyma at the uncinate process contained the tumor (double-headed arrow). ( b ) A photomicrograph showing a tumor with deep pancreatic invasion. The histopathologic DoI measurement was 20 mm.](https://storage.googleapis.com/dl.dentistrykey.com/clinical/ValidationofFeasibilityofMagneticResonanceImagingfortheMeasurementofDepthofTumorInvasioninDistalBileDuctCancerAccordingtotheNewAmericanJointCommitteeonCancerStagingSystem/5_1s20S1076633217303021.jpg)
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Vauthey J.N., Blumgart L.H.: Recent advances in the management of cholangiocarcinomas. Semin Liver Dis 1994; 14: pp. 109-114.
2. Shaib Y.H., El-Serag H.B., Davila J.A., et. al.: Risk factors of intrahepatic cholangiocarcinoma in the United States: a case-control study. Gastroenterology 2005; 128: pp. 620-626.
3. Hong S.M., Cho H., Moskaluk C.A., et. al.: Measurement of the invasion depth of extrahepatic bile duct carcinoma: an alternative method overcoming the current T classification problems of the AJCC staging system. Am J Surg Pathol 2007; 31: pp. 199-206.
4. Hong S.M., Kim M.J., Pi D.Y., et. al.: Analysis of extrahepatic bile duct carcinomas according to the New American Joint Committee on Cancer staging system focused on tumor classification problems in 222 patients. Cancer 2005; 104: pp. 802-810.
5. Chung Y.E., Kim M.J., Park Y.N., et. al.: Staging of extrahepatic cholangiocarcinoma. Eur Radiol 2008; 18: pp. 2182-2195.
6. Moon A., Choi D.W., Choi S.H., et. al.: Validation of T stage according to depth of invasion and N stage subclassification based on number of metastatic lymph nodes for distal extrahepatic bile duct (EBD) carcinoma. Medicine (Baltimore) 2015; 94: pp. e2064.
7. Ebata T., Nagino M., Nishio H., et. al.: Pancreatic and duodenal invasion in distal bile duct cancer: paradox in the tumor classification of the American Joint Committee on Cancer. World J Surg 2007; 31: pp. 2008-2015.
8. Edge S.B., Compton C.C.: The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol 2010; 17: pp. 1471-1474.
9. Min K.W., Kim D.H., Son B.K., et. al.: Invasion depth measured in millimeters is a predictor of survival in patients with distal bile duct cancer: decision tree approach. World J Surg 2017; 41: pp. 232-240.
10. Krasinskas A., Pawlik T.M., Mino-Kenudson M., et. al.: Distal bile duct.Amin M.B. et. al.AJCC cancer staging manual.2017.SpringerNew York, NY:pp. 317-325.
11. Joo I., Lee J.M.: Imaging bile duct tumors: pathologic concepts, classification, and early tumor detection. Abdom Imaging 2013; 38: pp. 1334-1350.
12. Park H.S., Lee J.M., Choi J.Y., et. al.: Preoperative evaluation of bile duct cancer: MRI combined with MR cholangiopancreatography versus MDCT with direct cholangiography. AJR Am J Roentgenol 2008; 190: pp. 396-405.
13. Sainani N.I., Catalano O.A., Holalkere N.S., et. al.: Cholangiocarcinoma: current and novel imaging techniques. Radiographics 2008; 28: pp. 1263-1287.
14. Hong S.M., Pawlik T.M., Cho H., et. al.: Depth of tumor invasion better predicts prognosis than the current American Joint Committee on Cancer T classification for distal bile duct carcinoma. Surgery 2009; 146: pp. 250-257.
15. Donner A., Zou G.: Testing the equality of dependent intraclass correlation coefficients. J Royal Stat Soc 2002; 51: pp. 367-379.
16. Altman D.: Inter-rater agreement. Pract Stat Med Res 1991; 5: pp. 403-409.
17. Hong S.M., Kang G.H., Lee H.Y., et. al.: Smooth muscle distribution in the extrahepatic bile duct: histologic and immunohistochemical studies of 122 cases. Am J Surg Pathol 2000; 24: pp. 660-667.
18. Group M.S.: Extramural depth of tumor invasion at thin-section MR in patients with rectal cancer: results of the MERCURY study. Radiology 2007; 243: pp. 132-139.
19. Sakamoto E., Nimura Y., Hayakawa N., et. al.: The pattern of infiltration at the proximal border of hilar bile duct carcinoma: a histologic analysis of 62 resected cases. Ann Surg 1998; 227: pp. 405-411.