
Rationale and Objectives
We sought to explore the image quality and diagnostic performance of virtual monochromatic imaging derived from dual-energy computed tomography coronary angiography (DE-CTCA) in patients with intermediate to high likelihood of coronary artery disease (CAD) and the influence of calcification.
Materials and Methods
Consecutive symptomatic patients with suspected CAD referred for invasive coronary angiography who underwent DE-CTCA and a coronary artery calcium scoring before the invasive procedure comprised the study population.
Results
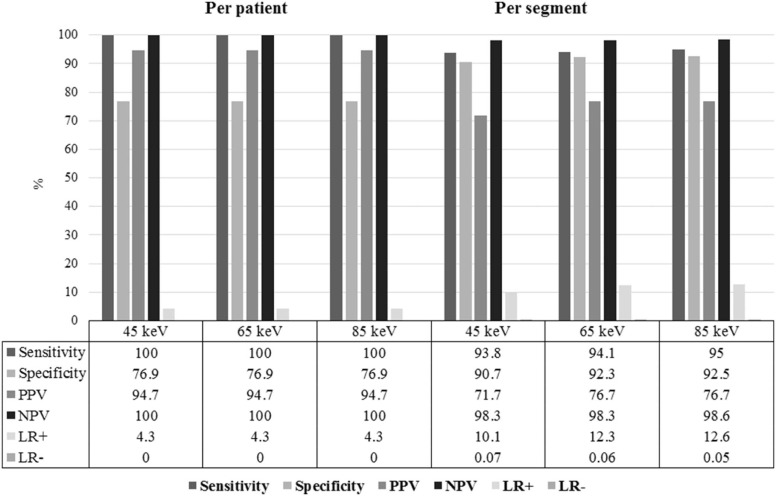
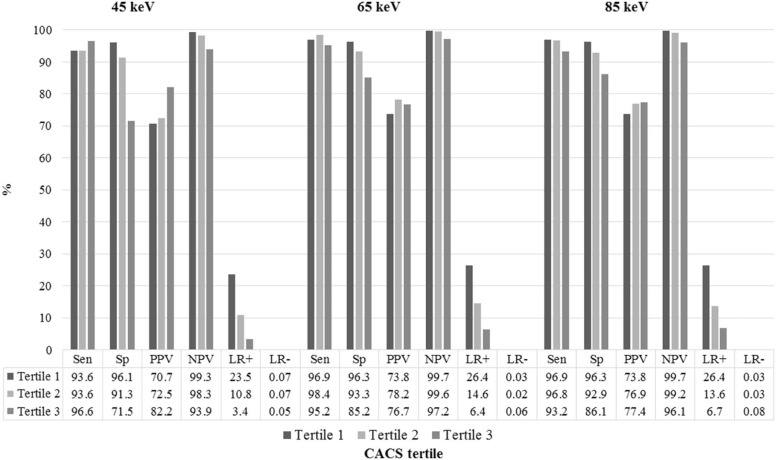
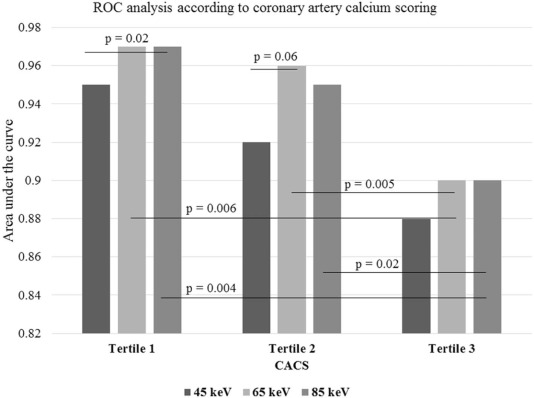
Sixty-seven patients were included. Image quality was significantly lower at 45 keV reconstructions (mean Likert score 45 keV 3.57 ± 0.6, 65 keV 4.07 ± 0.5, and 85 keV 4.09 ± 0.6; P < .0001). Patients with moderate calcification showed a trend toward a significant improvement in the diagnostic performance with 65 keV vs 45 keV reconstructions (45 keV, area under the curve 0.92 [95% confidence interval 0.89–0.95] vs 65 keV, area under the curve 0.96 [95% confidence interval 0.93–0.98], P = .06). The diagnostic performance of DE-CTCA was significantly lower in segments with higher coronary artery calcium scoring compared to segments with none or mild calcification, independent of the energy level applied.
Conclusions
In patients with intermediate to high likelihood of CAD, DE-CTCA had a good diagnostic performance, although significantly lower in segments with severe calcification.
Introduction
Computed tomography coronary angiography (CTCA) has been established as a valuable noninvasive diagnostic tool for the assessment of symptomatic patients with low to intermediate likelihood of coronary artery disease (CAD) . Notwithstanding, patients with intermediate to high likelihood of CAD have been consistently excluded from clinical studies involving this technology and consequently from diagnostic algorithms. To some extent, this has been attributed to the intricate distinction between heavily calcified plaques and luminal opacification that hamper the precise quantification of coronary stenosis . Calcified plaques usually seem larger on conventional single-energy computed tomography due to a number of technical issues such as blooming, beam hardening, and partial-volume effects, frequently leading to false-positive findings and therefore to potential unnecessary referral to invasive angiography .
Virtual monochromatic imaging derived from dual-energy computed tomography coronary angiography (DE-CTCA) shows promise to attenuate some of the aforementioned limitations and therefore might provide a more accurate assessment of high-risk patients . Briefly, the basic principle of DE-CTCA is the acquisition of two datasets from the same anatomic location with different kVp, which allows for synthesized monochromatic image reconstructions at different energy levels ranging from 40 to 140 keV. Although at the expense of higher image noise and blooming, lower energy levels yield higher intraluminal enhancement that allows a substantial iodine volume load reduction . In contrast, higher energy levels not only render a reduction in image noise and blooming but are also associated with significant reduction in luminal attenuation. We therefore sought to evaluate the image quality and diagnostic performance of DE-CTCA and the influence of different energy levels and extent of coronary calcification to accurately detect coronary stenosis in patients with intermediate to high likelihood of CAD.
Methods
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Image Acquisition
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Image Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Table 1
Demographical Characteristics ( n = 67)
N (%) Age (years ± SD) 61.3 ± 11.1 Male (%) 51(70%) Body mass index (kg/m 2 ) 28.3 ± 3.4 Diabetes (%) 14(21%) Hypertension (%) 47(70%) Hypercholesterolemia (%) 45(67%) Smoking (%) 38(57%) Previous myocardial infarction (%) 16(23%) Left ventricular ejection fraction (% ± SD) 57.3 ± 13.4 Systolic blood pressure (mmHg ± SD) 141.8 ± 21.8 Diastolic blood pressure (mmHg ± SD) 86.7 ± 13.0 Heart rate (bpm ± SD) 63.4 ± 8.3 Agatston calcium score (median, IQR) 597(184–1095)
bpm, beats per minute; IQR, interquartile range; SD, standard deviation.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusions
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Taylor A.J., Cerqueira M., Hodgson J.M., et. al.: ACCF/SCCT/ACR/AHA/ASE/ASNC/NASCI/SCAI/SCMR 2010 appropriate use criteria for cardiac computed tomography. A report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, the Society of Cardiovascular Computed Tomography, the American College of Radiology, the American Heart Association, the American Society of Echocardiography, the American Society of Nuclear Cardiology, the North American Society for Cardiovascular Imaging, the Society for Cardiovascular Angiography and Interventions, and the Society for Cardiovascular Magnetic Resonance. J Am Coll Cardiol 2010; 56: pp. 1864-1894.
2. Wright R.S., Anderson J.L., Adams C.D., et. al.: 2011 ACCF/AHA focused update incorporated into the ACC/AHA 2007 Guidelines for the Management of Patients with Unstable Angina/Non-ST-Elevation Myocardial Infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines developed in collaboration with the American Academy of Family Physicians, Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons. J Am Coll Cardiol 2011; 57: pp. e215-e367.
3. Hamm C.W., Bassand J.P., Agewall S., et. al.: ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: the task force for the management of acute coronary syndromes (ACS) in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J 2011; 32: pp. 2999-3054.
4. Brodoefel H., Burgstahler C., Tsiflikas I., et. al.: Dual-source CT: effect of heart rate, heart rate variability, and calcification on image quality and diagnostic accuracy. Radiology 2008; 247: pp. 346-355.
5. Meijboom W.B., Meijs M.F., Schuijf J.D., et. al.: Diagnostic accuracy of 64-slice computed tomography coronary angiography: a prospective, multicenter, multivendor study. J Am Coll Cardiol 2008; 52: pp. 2135-2144.
6. Ruzsics B., Lee H., Zwerner P.L., et. al.: Dual-energy CT of the heart for diagnosing coronary artery stenosis and myocardial ischemia-initial experience. Eur Radiol 2008; 18: pp. 2414-2424.
7. Carrascosa P.M., Deviggiano A., Capunay C., et. al.: Incremental value of myocardial perfusion over coronary angiography by spectral computed tomography in patients with intermediate to high likelihood of coronary artery disease. Eur J Radiol 2015; 84: pp. 637-642.
8. Carrascosa P., Capunay C., Rodriguez-Granillo G.A., et. al.: Substantial iodine volume load reduction in CT angiography with dual-energy imaging: insights from a pilot randomized study. Int J Cardiovasc Imaging 2014; 30: pp. 1613-1620.
9. Raju R., Thompson A.G., Lee K., et. al.: Reduced iodine load with CT coronary angiography using dual-energy imaging: a prospective randomized trial compared with standard coronary CT angiography. J Cardiovasc Comput Tomogr 2014; 8: pp. 282-288.
10. Genders T.S., Steyerberg E.W., Alkadhi H., et. al.: A clinical prediction rule for the diagnosis of coronary artery disease: validation, updating, and extension. Eur Heart J 2011; 32: pp. 1316-1330.
11. Leipsic J., Abbara S., Achenbach S., et. al.: SCCT guidelines for the interpretation and reporting of coronary CT angiography: a report of the Society of Cardiovascular Computed Tomography Guidelines Committee. J Cardiovasc Comput Tomogr 2014; 8: pp. 342-358.
12. Agatston A.S., Janowitz W.R., Hildner F.J., et. al.: Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol 1990; 15: pp. 827-832.
13. Halliburton S.S., Abbara S., Chen M.Y., et. al.: SCCT guidelines on radiation dose and dose-optimization strategies in cardiovascular CT. J Cardiovasc Comput Tomogr 2011; 5: pp. 198-224.
14. DeLong E.R., DeLong D.M., Clarke-Pearson D.L.: Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics 1988; 44: pp. 837-845.
15. Meijboom W.B., van Mieghem C.A., Mollet N.R., et. al.: 64-Slice computed tomography coronary angiography in patients with high, intermediate, or low pretest probability of significant coronary artery disease. J Am Coll Cardiol 2007; 50: pp. 1469-1475.
16. Arbab-Zadeh A., Miller J.M., Rochitte C.E., et. al.: Diagnostic accuracy of computed tomography coronary angiography according to pre-test probability of coronary artery disease and severity of coronary arterial calcification. The CORE-64 (Coronary Artery Evaluation Using 64-Row Multidetector Computed Tomography Angiography) International Multicenter Study. J Am Coll Cardiol 2012; 59: pp. 379-387.
17. Abdulla J., Pedersen K.S., Budoff M., et. al.: Influence of coronary calcification on the diagnostic accuracy of 64-slice computed tomography coronary angiography: a systematic review and meta-analysis. Int J Cardiovasc Imaging 2012; 28: pp. 943-953.
18. Yan R.T., Miller J.M., Rochitte C.E., et. al.: Predictors of inaccurate coronary arterial stenosis assessment by CT angiography. JACC Cardiovasc Imaging 2013; 6: pp. 963-972.
19. Carrascosa P.M., Cury R.C., Deviggiano A., et. al.: Comparison of myocardial perfusion evaluation with single versus dual-energy CT and effect of beam-hardening artifacts. Acad Radiol 2015; 22: pp. 591-599.
20. So A., Hsieh J., Li J.Y., et. al.: Beam hardening correction in CT myocardial perfusion measurement. Phys Med Biol 2009; 54: pp. 3031-3050.
21. Boll D.T., Merkle E.M., Paulson E.K., et. al.: Calcified vascular plaque specimens: assessment with cardiac dual-energy multidetector CT in anthropomorphically moving heart phantom. Radiology 2008; 249: pp. 119-126.
22. Secchi F., De Cecco C.N., Spearman J.V., et. al.: Monoenergetic extrapolation of cardiac dual energy CT for artifact reduction. Acta Radiol 2015; 56: pp. 413-418.
23. Obaid D.R., Calvert P.A., Gopalan D., et. al.: Dual-energy computed tomography imaging to determine atherosclerotic plaque composition: a prospective study with tissue validation. J Cardiovasc Comput Tomogr 2014; 8: pp. 230-237.
24. Scheske J.A., O’Brien J.M., Earls J.P., et. al.: Coronary artery imaging with single-source rapid kilovolt peak-switching dual-energy CT. Radiology 2013; 268: pp. 702-709.
25. Okayama S., Seno A., Soeda T., et. al.: Optimization of energy level for coronary angiography with dual-energy and dual-source computed tomography. Int J Cardiovasc Imaging 2012; 28: pp. 901-909.
26. Rodriguez-Granillo G.A., Carrascosa P., Cipriano S., et. al.: Myocardial signal density levels and beam-hardening artifact attenuation using dual-energy computed tomography. Clin Imaging 2015; 39: pp. 809-814.
27. Mancini G.B., Hartigan P.M., Shaw L.J., et. al.: Predicting outcome in the COURAGE trial (Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation): coronary anatomy versus ischemia. JACC Cardiovasc Interv 2014; 7: pp. 195-201.