
Rationale and Objectives
Fluoroscopy-guided lumbar puncture (FGLP) is a basic procedural component of radiology residency and neuroradiology fellowship training. Performance of the procedure with limited experience is associated with increased patient discomfort as well as increased radiation dose, puncture attempts, and complication rate. Simulation in health care is a developing field that has potential for enhancing procedural training. We demonstrate the design and utility of a virtual reality simulator for performing FGLP.
Materials and Methods
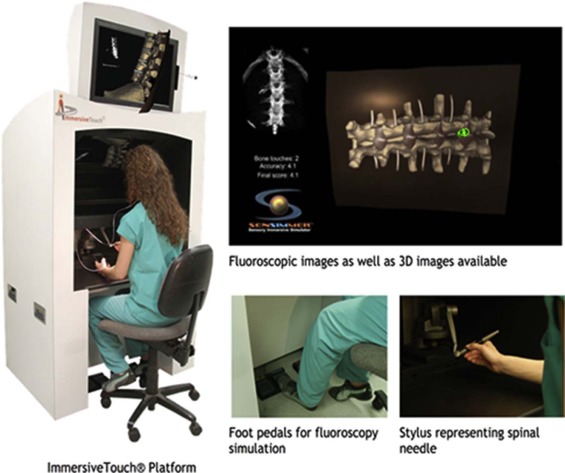
An FGLP module was developed on an ImmersiveTouch platform, which digitally reproduces the procedural environment with a hologram-like projection. From computed tomography datasets of healthy adult spines, we constructed a 3-D model of the lumbar spine and overlying soft tissues. We assigned different physical characteristics to each tissue type, which the user can experience through haptic feedback while advancing a virtual spinal needle. Virtual fluoroscopy as well as 3-D images can be obtained for procedural planning and guidance. The number of puncture attempts, the distance to the target, the number of fluoroscopic shots, and the approximate radiation dose can be calculated. Preliminary data from users who participated in the simulation were obtained in a postsimulation survey.
Results
All users found the simulation to be a realistic replication of the anatomy and procedure and would recommend to a colleague. On a scale of 1–5 (lowest to highest) rating the virtual simulator training overall, the mean score was 4.3 (range 3–5).
Conclusions
We describe the design of a virtual reality simulator for performing FGLP and present the initial experience with this new technique.
Introduction
Lumbar puncture (LP) is a commonly performed medical procedure for a variety of indications. Fluoroscopy-guided lumbar puncture (FGLP) is usually performed if attempts at the bedside are unsuccessful. There is also an increasing trend to perform LP under fluoroscopy without prior bedside attempts, such as for patients who are obese or have a difficult anatomy because of a prior spine surgery . In addition to higher success rates, fluoroscopic guidance may reduce the incidence of traumatic LP .
Performing a successful FGLP requires a combination of anatomic knowledge and technical skill. Although the anatomic knowledge is typically gained through conventional didactic methods, acquiring the technical expertise traditionally requires performing the procedure on a patient under close supervision initially, followed by a gradual transition to independency. For a minimally invasive procedure such as FGLP, serious complications are fortunately rare (less than 0.5%) ; however, performance of the procedure by an inexperienced operator requiring multiple attempts can be associated with increased patient discomfort as well as an increase in minor complications . Although cadavers have historically been used for procedural training, they are associated with increased costs and limited availability due to logistic problems of procurement, storage, and disposal. An alternative approach is using a physical task trainer in the form of a mannequin that can be modified to suit the purpose of training for LP. However, these devices have limited durability, and it may not be practical or cost-effective to create or purchase multiple models as may be needed to represent different case difficulty levels. Also, utilizing a mannequin in a fluoroscopy room during the simulated procedure requires additional personnel exposure to radiation and resource utilization.
Get Radiology Tree app to read full this article<
Materials and Methods
Get Radiology Tree app to read full this article<
Virtual Fluoroscopy-guided Lumbar Puncture Module Design
Get Radiology Tree app to read full this article<
Using the Virtual Fluoroscopy-guided Lumbar Puncture Module
Get Radiology Tree app to read full this article<

Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Preliminary Data
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
TABLE 1
Postsimulation Survey
Participant 1 2 3 4 5 6 Experience: training level Nurse practitioner PGY-2 PGY-5 PGY-5 PGY-6 PGY-7 Experience: number of prior FGLPs performed 0 1–5 16–20 16–20 1–5 6–10 How important is it for the simulation module to realistically replicate anatomy visually and through haptic feedback? Very important Very important Extremely important Extremely important Very important Very important How realistic was the anatomy visually? Realistic Extremely realistic Very realistic Somewhat realistic Very realistic Somewhat realistic How realistic was the system in providing tactile feedback? N/A (no prior LP experience) Realistic Realistic Somewhat realistic Realistic Somewhat realistic Overall rating (1–5) 5 5 4 5 3 4 Recommend to colleague (yes/no) Yes Yes Yes Yes Yes Yes
FGLP, fluoroscopy-guided lumbar puncture; LP, lumbar puncture; N/A, not applicable; PGY, Post-graduate Year.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgment
Get Radiology Tree app to read full this article<
References
1. Kroll H., Duszak R., Nsiah E., et. al.: Trends in lumbar puncture over 2 decades: a dramatic shift to radiology. AJR Am J Roentgenol 2015; 204: pp. 15-19.
2. Shah K.H., McGillicuddy D., Spear J., et. al.: Predicting difficult and traumatic lumbar punctures. Am J Emerg Med 2007; 25: pp. 608-611.
3. Lammers R.L.: Competence of new emergency medicine residents in the performance of lumbar punctures. Acad Emerg Med 2005; 12: pp. 622-628.
4. Eskey C.J., Ogilvy C.S.: Fluoroscopy-guided lumbar puncture: decreased frequency of traumatic tap and implications for the assessment of CT-negative acute subarachnoid hemorrhage. AJNR Am J Neuroradiol 2001; 22: pp. 571-576.
5. Evans R.W.: Complications of lumbar puncture. Neurol Clin 1998; 16: pp. 83-105.
6. Ruff R.L., Dougherty J.H.: Complications of lumbar puncture followed by anticoagulation. Stroke 1981; 12: pp. 879-881.
7. Baer E.T.: Post-dural puncture bacterial meningitis. Anesthesiology 2006; 105: pp. 381-393.
8. Nigrovic L.E., Kuppermann N., Neuman M.I.: Risk factors for traumatic or unsuccessful lumbar punctures in children. Ann Emerg Med 2007; 49: pp. 762-771.
9. Alaraj A., Luciano C.J., Bailey D.P., et. al.: Virtual reality cerebral aneurysm clipping simulation with real-time haptic feedback. Neurosurgery 2015; 11: pp. 52-58.
10. Issenberg S.B., McGaghie W.C., Petrusa E.R., et. al.: Features and uses of high-fidelity medical simulations that lead to effective learning: a BEME systematic review. Med Teach 2005; 27: pp. 10-28.
11. Kirkman M.A.: Deliberate practice, domain-specific expertise, and implications for surgical education in current climes. J Surg Educ 2013; 70: pp. 309-317.
12. de Oliveira Filho G.L.R.: The construction of learning curves for basic skills in anesthetic procedures: an application for the cumulative sum method. Anesth Analg 2002; 95: pp. 411-416.
13. Lemole G.M., Banerjee P.P., Luciano C., et. al.: Virtual reality in neurosurgical education. Neurosurgery 2007; 61: pp. 142-149.
14. The Accreditation Council for Graduate Medical Education : The American Board of Radiology. The Diagnostic Radiology Milestone Project2015.
15. Yang H., Schaffer K., Liu L., et. al.: Benchmarking lumbar puncture fluoroscopy time during fellowship training. AJNR Am J Neuroradiol 2017; 38: pp. 656-658.
16. Boddu S.R., Corey A., Peterson R., et. al.: Fluoroscopic-guided lumbar puncture: fluoroscopic time and implications of body mass index—a baseline study. AJNR Am J Neuroradiol 2014; 35: pp. 1475-1480.