
Rationale and Objectives
To retrospectively determine the value of a volumetric ventricle analysis for the assessment of right ventricular dysfunction in patients with suspected pulmonary embolism (PE) by using image data from non-electrocardiographically (ECG)-gated multidetector computed tomography angiography (CTA).
Materials and Methods
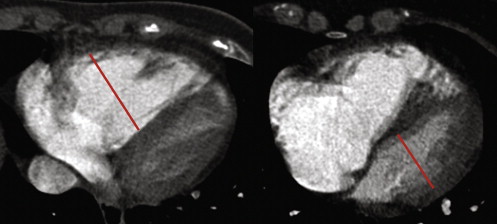
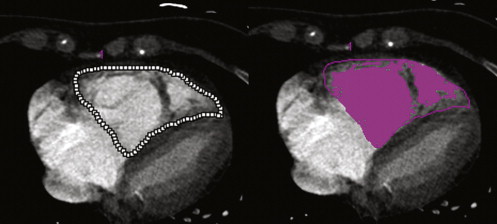
Hypothesizing that the presence of PE and the embolus location correlated with right ventricular dysfunction, we retrospectively analyzed 100 non–ECG-gated pulmonary CTA datasets of patients with central, peripheral, and without PE. Right ventricle/left ventricle (RV/LV) diameter ratio measured in transverse sections (RV/LV trans ), four-chamber view (RV/LV 4ch ), and RV/LV volume ratio (RV/LV vol ) were assessed on CT images. The results were correlated with the embolus location, the 30-day mortality rate, and the necessity of intensive care treatment.
Results
All CT parameters showed statistically significant differences between all patients groups depended on embolus location. The receiver operating characteristic analysis RV/LV vol showed the strongest discriminatory power to differ between patients with central and without PE and between patients with central and peripheral PE (central PE vs. no PE: RV/LV vol = 0.932, RV/LV trans = 0.880, and RV/LV 4ch = 0.811, central PE vs. peripheral PE: RV/LV vol = 0.950, RV/LV trans = 0.849, and RV/LV 4ch = 0.881), indicating a correlation with embolus location predisposing for RVD. For the identification of high-risk patients with PE all three CT parameters showed statistically significant values ( P < .0001), whereas in the receiver operating characteristic analysis, RV/LV vol had the strongest discriminatory power (RV/LV vol = 0.819, RV/LV trans = 0.799, and RV/LV 4ch = 0.758).
Conclusion
Ventricle volumetry of non–ECG-gated CTA allows the assessment of right ventricular dysfunction in patients with acute PE. Compared to unidimensional measurements, a volumetric analysis seems to be slightly superior to identify high-risk patients with adverse clinical outcome. However, the method is more time consuming and requires dedicated software tools compared to unidimensional parameters, which is disadvantageous in an emergency setting.
Acute pulmonary embolism (PE) is a common disease with a variable prognosis that ranges from incidental clinical unimportant small embolism to massive embolism with sudden death . If undiagnosed, PE is fatal in up to 30%, but even if diagnosed the 30-day mortality rate reaches 10% . Right ventricular dysfunction (RVD) is the major prognostic factor in patients with acute PE . Patients with RVD have a higher mortality rate than those without RVD, even if they are hemodynamically stable at clinical presentation . Therefore, the identification of patients with RVD is of major clinical importance, because these patients might benefit from intensive therapy with thrombolytic agents or surgery embolectomy . Echocardiography is the standard of reference for the assessment of RVD in patients with PE , but is operator dependent.
Multidetector computed tomography angiography (CTA) of the pulmonary arteries has become the accepted gold standard for the diagnosis of acute PE . In addition to the detection of PE, CTA also allows assessing the dimensions of the cardiac chambers, which are displayed in the same examination. Because of this, many investigators have tried to identify quantitative CT parameters for the assessment of RVD . Several studies have demonstrated that similar to echocardiography simple measurements of the maximum right ventricular (RV) to left ventricular (LV) dimension ratio (RV/LV) can be used to identify RVD in patients with acute PE .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Patients and Study Design
Get Radiology Tree app to read full this article<
Imaging Protocol
Get Radiology Tree app to read full this article<
CT Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Clinical Outcome
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Clinical Outcome
Get Radiology Tree app to read full this article<
CT Parameters and Embolus Location
Get Radiology Tree app to read full this article<
Table 1
Clinical Characteristics of the 22 High-risk Patients
Death 4 Resuscitation 8 Systemic lysis therapy 8 Cardiogenic shock 10 Catecholamine dependent 10 Mechanical ventilation 10 Echocardiographic-confirmed severe right heart failure 16
Note: Some patients met several high risk criteria.
Table 2
Means, ▵ of Means, and t -test of Different CT Parameters to Differentiate Patient Groups Dependent on Embolus Location
Central vs. Peripheral PE Means ▵P Values RV/LV trans 1.25 vs. 0.88 0.37 <.0001 RV/LV 4ch 1.20 vs. 0.87 0.33 <.0001 RV/LV vol 1.65 vs. 0.86 0.79 <.0001 Central vs. no PE RV/LV trans 1.25 vs. 0.83 0.42 <.0001 1.20 vs. 0.84 0.36 <.0001 RV/LV vol 1.65 vs. 0.83 0.82 <.0001 Peripheral vs. no PE RV/LV trans 0.88 vs. 0.83 0.05 <.0001 RV/LV 4ch 0.87 vs. 0.84 0.03 <.0001 RV/LV vol 0.86 vs. 0.83 0.03 <.0001
CT: computed tomography; RV/LV trans : right ventricle/left ventricle diameter ratio measured in transverse sections; RV/LV 4ch : four-chamber view; RV/LV vol : RV/LV volume ratio; PE: pulmonary embolism.
Table 3
ROC Analysis of CT Parameters to Evaluate the Discriminatory Power to Differentiate Patient Groups Dependent on Embolus Location
Central vs. Peripheral Central vs. No Peripheral vs. No RV/LV trans 0.811 0.849 0.582 RV/LV 4ch 0.880 0.881 0.532 RV/LV vol 0.932 0.950 0.587
CT: computed tomography; RV/LV trans : right ventricle/left ventricle diameter ratio measured in transverse sections; RV/LV 4ch : four-chamber view; RV/LV vol : RV/LV volume ratio.
Get Radiology Tree app to read full this article<
CT Parameter and Patients Outcome
Get Radiology Tree app to read full this article<
Table 4
Means, ▵ of Means and t -test of Different CT Parameters to Identify High-risk Patients
Means High-risk Group vs. Other Patients ▵P Values RV/LV trans 1.27 vs. 0.89 0.38 <.0001 RV/LV 4ch 1.18 vs. 0.90 0.28 <.0001 RV/LV vol 1.68 vs. 0.93 0.79 <.0001
CT: computed tomography; RV/LV trans : right ventricle/left ventricle diameter ratio measured in transverse sections; RV/LV 4ch : four-chamber view; RV/LV vol : RV/LV volume ratio.
Table 5
ROC Analysis of the Different CT Parameters to Identify High-risk Patients
RV/LV trans 0.799 RV/LV 4ch 0.758 RV/LV vol 0.819
ROC: receiver operating characteristic; CT: computed tomography; RV/LV trans : right ventricle/left ventricle diameter ratio measured in transverse sections; RV/LV 4ch : four-chamber view; RV/LV vol : RV/LV volume ratio.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Postprocessing Time for the Volumetric Analysis
Get Radiology Tree app to read full this article<
Radiation Dose
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Goldhaber S.Z.: Pulmonary embolism. N Engl J Med 1998; 339: pp. 93-104.
2. Bell W.R., Simon T.L.: Current status of pulmonary thromboembolic disease: pathophysiology, diagnosis, prevention, and treatment. Am Heart J 1982; 103: pp. 239-262.
3. Goldhaber S.Z., Visani L., De Rosa M.: Acute pulmonary embolism: clinical outcomes in the International Cooperative Pulmonary Embolism Registry (ICOPER). Lancet 1999; 353: pp. 1386-1389.
4. Wood K.E.: Major pulmonary embolism: review of a pathophysiologic approach to the golden hour of hemodynamically significant pulmonary embolism. Chest 2002; 121: pp. 877-905.
5. Grifoni S., Olivotto I., Cecchini P., et. al.: Short-term clinical outcome of patients with acute pulmonary embolism, normal blood pressure, and echocardiographic right ventricular dysfunction. Circulation 2000; 101: pp. 2817-2822.
6. Kreit J.W.: The impact of right ventricular dysfunction on the prognosis and therapy of normotensive patients with pulmonary embolism. Chest 2004; 125: pp. 1539-1545.
7. Leacche M., Unic D., Goldhaber S.Z., et. al.: Modern surgical treatment of massive pulmonary embolism: results in 47 consecutive patients after rapid diagnosis and aggressive surgical approach. J Thorac Cardiovasc Surg 2005; 129: pp. 1018-1023.
8. Goldhaber S.Z.: Echocardiography in the management of pulmonary embolism. Ann Intern Med 2002; 136: pp. 691-700.
9. Kasper W., Konstantinides S., Geibel A., et. al.: Prognostic significance of right ventricular afterload stress detected by echocardiography in patients with clinically suspected pulmonary embolism. Heart 1997; 77: pp. 346-349.
10. Vieillard-Baron A., Page B., Augarde R., et. al.: Acute cor pulmonale in massive pulmonary embolism: incidence, echocardiographic pattern, clinical implications and recovery rate. Intensive Care Med 2001; 27: pp. 1481-1486.
11. Stein P.D., Fowler S.E., Goodman L.R., et. al.: Multidetector computed tomography for acute pulmonary embolism. N Engl J Med 2006; 354: pp. 2317-2327.
12. Kelly A.M., Patel S., Carlos R.C., et. al.: Multidetector row CT pulmonary angiography and indirect venography for the diagnosis of venous thromboembolic disease in intensive care unit patients. Acad Radiol 2006; 13: pp. 486-495.
13. Weiss C.R., Scatarige J.C., Diette G.B., et. al.: CT pulmonary angiography is the first-line imaging test for acute pulmonary embolism: a survey of US clinicians. Acad Radiol 2006; 13: pp. 434-446.
14. Dogan H., Kroft L.J., Huisman M.V., et. al.: Right ventricular function in patients with acute pulmonary embolism: analysis with electrocardiography-synchronized multi-detector row CT. Radiology 2007; 242: pp. 78-84.
15. Contractor S., Maldjian P.D., Sharma V.K., et. al.: Role of helical CT in detecting right ventricular dysfunction secondary to acute pulmonary embolism. J Comput Assist Tomogr 2002; 26: pp. 587-591.
16. Groves A.M., Win T., Charman S.C., et. al.: Semi-quantitative assessment of tricuspid regurgitation on contrast-enhanced multidetector CT. Clin Radiol 2004; 59: pp. 715-719.
17. Mastora I., Remy-Jardin M., Masson P., et. al.: Severity of acute pulmonary embolism: evaluation of a new spiral CT angiographic score in correlation with echocardiographic data. Eur Radiol 2003; 13: pp. 29-35.
18. Qanadli S.D., El Hajjam M., Vieillard-Baron A., et. al.: New CT index to quantify arterial obstruction in pulmonary embolism: comparison with angiographic index and echocardiography. AJR Am J Roentgenol 2001; 176: pp. 1415-1420.
19. Quiroz R., Kucher N., Schoepf U.J., et. al.: Right ventricular enlargement on chest computed tomography: prognostic role in acute pulmonary embolism. Circulation 2004; 109: pp. 2401-2404.
20. Reid J.H.: Semi-quantitative assessment of tricuspid regurgitation on contrast-enhanced multidetector CT. Clin Radiol 2004; 59: pp. 713-714.
21. Reid J.H., Murchison J.T.: Acute right ventricular dilatation: a new helical CT sign of massive pulmonary embolism. Clin Radiol 1998; 53: pp. 694-698.
22. Bankier A.A., Janata K., Fleischmann D., et. al.: Severity assessment of acute pulmonary embolism with spiral CT: evaluation of two modified angiographic scores and comparison with clinical data. J Thorac Imaging 1997; 12: pp. 150-158.
23. Mansencal N., Joseph T., Vieillard-Baron A., et. al.: Diagnosis of right ventricular dysfunction in acute pulmonary embolism using helical computed tomography. Am J Cardiol 2005; 95: pp. 1260-1263.
24. Schoepf U.J., Kucher N., Kipfmueller F., et. al.: Right ventricular enlargement on chest computed tomography: a predictor of early death in acute pulmonary embolism. Circulation 2004; 110: pp. 3276-3280.
25. Araoz P.A., Gotway M.B., Trowbridge R.L., et. al.: Helical CT pulmonary angiography predictors of in-hospital morbidity and mortality in patients with acute pulmonary embolism. J Thorac Imaging 2003; 18: pp. 207-216.
26. Mansencal N., Joseph T., Vieillard-Baron A., et. al.: Comparison of different echocardiographic indexes secondary to right ventricular obstruction in acute pulmonary embolism. Am J Cardiol 2003; 92: pp. 116-119.
27. Schoepf U.J., Costello P.: CT angiography for diagnosis of pulmonary embolism: state of the art. Radiology 2004; 230: pp. 329-337.
28. Schertler T., Frauenfelder T., Stolzmann P., et. al.: Triple rule-out CT in patients with suspicion of acute pulmonary embolism: findings and accuracy. Acad Radiol 2009; 16: pp. 708-717.
29. Ghaye B., Ghuysen A., Willems V., et. al.: Severe pulmonary embolism: pulmonary artery clot load scores and cardiovascular parameters as predictors of mortality. Radiology 2006; 239: pp. 884-891.
30. Lu M.T., Ersoy H., Whitmore A.G., et. al.: Reformatted four-chamber and short-axis views of the heart using thin section (</ = 2 mm) MDCT images. Acad Radiol 2007; 14: pp. 1108-1112.
31. Mayo J.R., Aldrich J., Muller N.L.: Radiation exposure at chest CT: a statement of the Fleischner Society. Radiology 2003; 228: pp. 15-21.
32. Araoz P.A., Gotway M.B., Harrington J.R., et. al.: Pulmonary embolism: prognostic CT findings. Radiology 2007; 242: pp. 889-897.
33. Ghuysen A., Ghaye B., Willems V., et. al.: Computed tomographic pulmonary angiography and prognostic significance in patients with acute pulmonary embolism. Thorax 2005; 60: pp. 956-961.
34. van der Meer R.W., Pattynama P.M., van Strijen M.J., et. al.: Right ventricular dysfunction and pulmonary obstruction index at helical CT: prediction of clinical outcome during 3-month follow-up in patients with acute pulmonary embolism. Radiology 2005; 235: pp. 798-803.
35. Einstein A.J., Henzlova M.J., Rajagopalan S.: Estimating risk of cancer associated with radiation exposure from 64-slice computed tomography coronary angiography. JAMA 2007; 298: pp. 317-323.
36. Johnson T.R., Nikolaou K., Becker A., et. al.: Dual-source CT for chest pain assessment. Eur Radiol 2008; 18: pp. 773-780.
37. Rahmani N., Jeudy J., White C.S.: Triple rule-out and dedicated coronary artery CTA: comparison of coronary artery image quality. Acad Radiol 2009; 16: pp. 604-609.
38. Aujesky D., Jimenez D., Mor M.K., et. al.: Weekend versus weekday admission and mortality after acute pulmonary embolism. Circulation 2009; 119: pp. 962-968.