
Rationale and Objectives
To perform a retrospective, quantitative assessment of the anatomic relationship between intra-axial, supratentorial, primary brain tumors, and adjacent white matter fiber tracts based on anatomic and diffusion tensor magnetic resonance imaging (MRI). We hypothesized that white matter infiltration may be common among different types of tumor.
Material and Methods
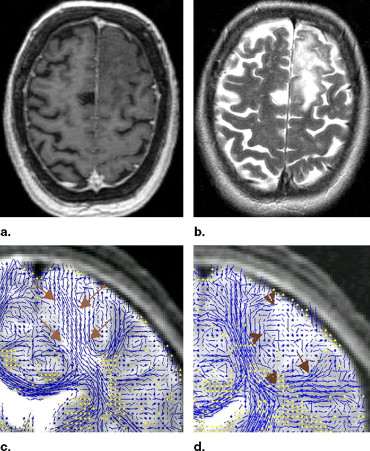
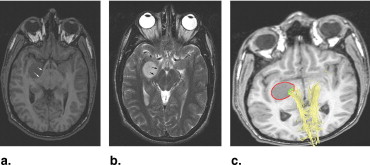
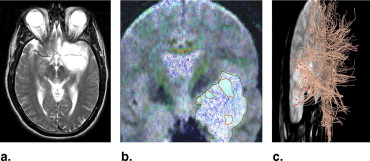
Preoperative, anatomic (T1- and T2-weighted), and LINESCAN diffusion tensor MRI were obtained in 12 patients harboring supratentorial gliomas (World Health Organization [WHO] Grades II and III). The two imaging modalities were rigidly registered. The tumors were manually segmented from the T1- and T2-weighted MRI, and their volume calculated. A three-dimensional tractography was performed in each case. A second segmentation and volume measurement was performed on the tumor regions intersecting adjacent white matter fiber tracts. Statistical methods included summary statistics to examine the fraction of tumor volume infiltrating adjacent white matter.
Results
There were five patients with low-grade oligodendroglioma (WHO Grade II), one with low-grade mixed oligoastrocytoma (WHO Grade II), one with ganglioglioma, two with low-grade astrocytoma (WHO Grade II), and three with anaplastic astrocytoma (WHO Grade III). We identified white matter tracts infiltrated by tumor in all 12 cases. The median tumor volume (± standard deviation) in our patient population was 42.5 ± 28.9 mL. The median tumor volume (± standard deviation) infiltrating white matter fiber tracts was 5.2 ± 9.9 mL. The median percentage of tumor volume infiltrating white matter fiber tracts was 21.4% ± 9.7%.
Conclusions
The information provided by diffusion tensor imaging combined with anatomic MRI might be useful for neurosurgical planning and intraoperative guidance. Our results confirm previous reports that extensive white matter infiltration by primary brain tumors is a common occurrence. However, prospective, large population studies are required to definitively clarify this issue, and how infiltration relates to histologic tumor type, tumor size, and location.
According to the Central Brain Tumor Registry of the United States, the incidence of primary benign and malignant brain tumors in this country is 14.1 patients per 100,000 individuals per year (6.8 per 100,000 individuals per year for low-grade tumors, and 7.3 per 100,000 individuals per year for malignant tumors) ( ).
The survival of patients harboring primary brain tumors appears to be influenced by a variety of factors, such as age, histologic tumor type, gender, preoperative Karnofsky performance score, epilepsy as presenting symptom, tumor involvement of the contralateral hemisphere, and extent of tumor resection ( ).
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and methods
Patient Population
Get Radiology Tree app to read full this article<
Table 1
Patient Population and Tumor Characteristics
Case No. Sex, Age (y) Tumor Location Histopathology Eloquent Cortical and White Matter Areas Affected 1 F 33 L frontal Astrocytoma WHO II SMA, motor strip, motor pathway 2 F 34 R temporal Oligodendroglioma WHO II Wernicke’s area, optic radiation 3 F 62 L frontal Oligodendroglioma WHO II SMA, motor pathway 4 M 62 R frontal medial Anaplastic Astrocytoma Motor strip, motor pathway 5 M 38 L frontal Astrocytoma WHO II Motor strip, motor pathway 6 F 45 L fronto-parietal Anaplastic Astrocytoma Motor and sensory strip, motor pathway, arcuate (superior longitudinal) fasciculus 7 F 46 R occipital Oligodendroglioma WHO II Optic radiation 8 M 23 R insular Ganglioglioma Motor pathway, uncinate fasciculus 9 F 18 R frontal Anaplastic Astrocytoma (WHO III) Motor strip, motor pathway 10 M 49 L frontal Oligodendroglioma WHO II SMA, motor pathway, corpus callosum 11 M 47 L fronto-temporal Mixed Oligoastrocytoma WHO II Broca’s area, uncinate fasciculus 12 F 56 L fronto-parietal Oligodendroglioma WHO II Motor and sensory strip, motor pathway, arcuate fasciculus
WHO: World Health Organization; SMA: Supplementary Motor Area.
Get Radiology Tree app to read full this article<
Image Acquisition
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Diffusion Tensor Imaging
Get Radiology Tree app to read full this article<
Image Analysis
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Table 2
Volumetric Assessment of White Matter Infiltration
Case No. Tumor Volume (mL) Tumor Volume Infiltrating Fiber Tracts (mL) Fraction of Tumor Volume Infiltrating Fiber Tracts (% of Total Tumor Volume) 1 33.7 4.8 14.2 2 51.3 13.7 26.7 3 32.3 2.4 7.4 4 9.3 2.6 28.0 5 28.3 3.5 12.4 6 62.6 23.1 36.9 7 9.2 2.6 28.3 8 13.0 2.0 15.4 9 91.8 22.6 24.6 10 87.7 30.7 35.0 11 52.8 5.7 10.8 12 70 12.8 18.3
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Central Brain Tumor Registry of the United States. Primary brain tumors in The United States 1998–2002. Statistical report: primary brain tumors in the United States 1998–2002 available online at: http://cbtrus.org/reports//2005-2006/2006report.pdf . Accessed February 11, 2007.
2. Nicolato A., Gerosa M.A., Fina P., et. al.: Prognostic factors in low-grade supratentorial astrocytomas: a uni-multivariate statistical analysis in 76 surgically treated adult patients. Surg Neurol 1995; 44: pp. 208-223.
3. Pignatti F., van den Bent M., Curran D., et. al.: Prognostic factors for survival in adult patients with cerebral low-grade glioma. J Clin Oncol 2002; 20: pp. 2076-2084.
4. Janny P., Cure H., Mohr M., et. al.: Low grade supratentorial astrocytomas. Cancer 1994; 73: pp. 1937-1945.
5. Keles G.E., Lamborn K.R., Berger M.S.: Low-grade hemispheric gliomas in adults: a critical review of extent of resection as a factor influencing outcome. J Neurosurg 2001; 95: pp. 735-745.
6. Claus E.B., Black P.M.: Survival rates and patterns of care for patients diagnosed with supratentorial low-grade gliomas: data from the SEER program, 1973–2001. Cancer 2006; 106: pp. 1358-1363.
7. Mori S., van Zijl P.C.: Fiber tracking: principles and strategies—a technical review. NMR Biomed 2002; 15: pp. 468-480.
8. Lowe M.J., Horenstein C., Hirsch J.G., et. al.: Functional pathway-defined MRI diffusion measures reveal increased transverse diffusivity of water in multiple sclerosis. Neuroimage 2006; 32: pp. 1127-1133.
9. Kealey S.M., Kim Y., Whiting W.L., et. al.: Determination of multiple sclerosis plaque size with diffusion-tensor MR imaging: comparison study with healthy volunteers. Radiology 2005; 236: pp. 615-620.
10. Witwer B.P., Moftakhar R., Hasan K.M., et. al.: Diffusion-tensor imaging of white matter tracts in patients with cerebral neoplasm. J Neurosurg 2002; 97: pp. 568-575.
11. Mori S., Frederiksen K., van Zijl P.C., et. al.: Brain white matter anatomy of tumor patients evaluated with diffusion tensor imaging. Ann Neurol 2002; 51: pp. 377-380.
12. Inoue T., Ogasawara K., Beppu T., et. al.: Diffusion tensor imaging for preoperative evaluation of tumor grade in gliomas. Clin Neurol Neurosurg 2005; 107: pp. 174-180.
13. Goebell E., Paustenbach S., Vaeterlein O., et. al.: Low-grade and anaplastic gliomas: differences in architecture evaluated with diffusion-tensor MR imaging. Radiology 2006; 239: pp. 217-222.
14. Mandonnet E., Capelle L., Duffau H.: Extension of paralimbic low grade gliomas: toward an anatomical classification based on white matter invasion patterns. J Neurooncol 2006; 78: pp. 179-185.
15. Gering D.T., Nabavi A., Kikinis R., et. al.: An integrated visualization system for surgical planning and guidance using image fusion and an open MR. J Magn Reson Imaging 2001; 13: pp. 967-975.
16. Wells W.M., Viola P., Atsumi H., et. al.: Multi-modal volume registration by maximization of mutual information. Med Image Anal 1996; 1: pp. 35-51.
17. West J., Fitzpatrick J.M., Wang M.Y., et. al.: Comparison and evaluation of retrospective intermodality brain image registration techniques. J Comput Assist Tomogr 1997; 21: pp. 554-566.
18. Nimsky C., Fujita A., Ganslandt O., et. al.: Volumetric assessment of glioma removal by intraoperative high-field magnetic resonance imaging. Neurosurgery 2004; 55: pp. 358-701.
19. Daumas-Duport C., Varlet P., Tucker M.L., et. al.: Oligodendrogliomas. J Neurooncol 1997; 34: pp. 37-59.
20. Kelly P.J., Daumas-Duport C., Kispert D.B., et. al.: Imaging-based stereotaxic serial biopsies in untreated intracranial glial neoplasms. J Neurosurg 1987; 66: pp. 865-874.
21. Price S.J., Jena R., Burnet N.G., et. al.: Improved delineation of glioma margins and regions of infiltration with the use of diffusion tensor imaging: an image-guided biopsy study. AJNR Am J Neuroradiol 2006; 27: pp. 1969-1974.
22. Provenzale J.M., McGraw P., Mhatre P., et. al.: Peritumoral brain regions in gliomas and meningiomas: investigation with isotropic diffusion-weighted MR imaging and diffusion-tensor MR imaging. Radiology 2004; 232: pp. 451-460.
23. Peled S., Gudbjartsson H., Westin C.F., et. al.: Magnetic resonance imaging shows orientation and asymmetry of white matter fiber tracts. Brain Res 1998; 780: pp. 27-33.
24. Westin C.F., Maier S.E., Mamata H., et. al.: Processing and visualization for diffusion tensor MRI. Med Image Anal 2002; 6: pp. 93-108.
25. Ojemann J.G., Miller J.W., Silbergeld D.L.: Preserved function in brain invaded by tumor. Neurosurgery 1996; 39: pp. 253-259.
26. Schiffbauer H., Berger M.S., Ferrari P., et. al.: Preoperative magnetic source imaging for brain tumor surgery: a quantitative comparison with intraoperative sensory and motor mapping. J Neurosurg 2002; 97: pp. 1333-1342.
27. Skirboll S.S., Ojemann G.A., Berger M.S., et. al.: Functional cortex and subcortical white matter located within gliomas. Neurosurgery 1996; 38: pp. 678-685.
28. Nimsky C., Ganslandt O., Fahlbusch R.: Implementation of fiber tract navigation. Neurosurgery 2006; 58: pp. ONS292-ONS304.
29. Talos I.F., Zou K.H., Ohno-Machado L., et. al.: Supratentorial low-grade glioma resectability: statistical predictive analysis based on anatomic MR features and tumor characteristics. Radiology 2006; 239: pp. 506-513.