
Rationale and Objectives
To (1) apply a quantitative volumetric textural analysis (VTA) to colorectal masses at CT colonography (CTC) for the differentiation of malignant and benign lesions and to (2) compare VTA with human performance.
Materials and Methods
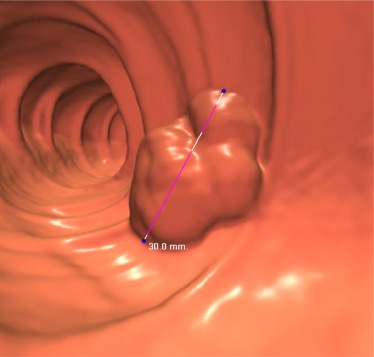
A validated, quantitative VTA method was applied to 63 pathologically proven colorectal masses (mean size, 4.2 cm; range, 3–8 cm) at noncontrast CTC in 59 adults (mean age, 66.5 years; range, 45.9–91.6 years). Fifty-one percent (32/63) of the masses were invasive adenocarcinoma, and the remaining 49% (31/63) were large benign adenomas. Three readers with CTC experience independently assessed the likelihood of malignancy using a 5-point scale (1 = definitely benign, 2 = probably benign, 3 = indeterminate, 4 = probably malignant, 5 = definitely malignant). Areas under the curve (AUCs) and accuracy levels were compared.
Results
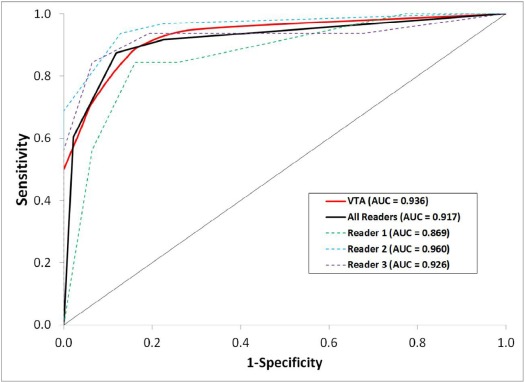
VTA achieved optimal sensitivity of 83.6% vs 91.7% for human readers ( P = .034), with specificities of 87.5% and 77.4%, respectively ( P = .007). No significant difference in overall accuracy was seen between VTA and human readers (85.5% vs 84.7%, P = .753). The AUC for differentiating benign and malignant lesions was 0.936 for VTA and 0.917 for human readers. Intraclass correlation coefficient among the human readers was 0.76, indicating good to excellent agreement.
Conclusion
VTA demonstrates excellent performance for distinguishing benign from malignant colorectal masses (≥3 cm) at CTC, comparable yet potentially complementary to experienced human performance.
Introduction
Colorectal cancer (CRC) remains a major public health issue in the United States, with recent figures estimating nearly 135,000 new diagnoses and 50,000 deaths per year . Fortunately, CRC is generally believed to begin as a benign colorectal polyp, with most requiring many years to progress to invasive cancer . The detection and removal of these benign precursors prior to malignant transformation through screening programs remains the cornerstone of CRC prevention . Over the last 10–15 years, CT colonography (CTC) has emerged as a validated CRC screening tool, recently gaining US Preventative Services Task Force approval as a recommended CRC screening test . CTC is comparable in effectiveness to traditional optical colonoscopy (OC) for the detection of advanced colorectal neoplasia and has the advantages of being noninvasive, cost-effective , and less operator dependent .
Historically, distinguishing large benign colorectal precursor mass lesions from truly invasive malignant cancers has presented a challenge both at CTC and at OC. A large degree of overlap exists between large advanced benign and malignant lesions with regard to observable features of lesion appearance (eg, size and morphology). Consequently, the standard of care for screening CTC is to send all large polyps (diameter ≥10 mm) for polypectomy, whereas the management of small (6–9 mm) lesions can be individualized between polypectomy and CTC surveillance . The standard of care for screening OC has generally been to remove all polyps regardless of size, although some have deviated from this practice. However, recent studies have reinforced that not all benign neoplastic polyps—even those of identical histologic subtype—present the same risk for growth and malignant transformation , and the search for novel methods to predict polyp behavior remains an active area of research.
Get Radiology Tree app to read full this article<
Materials and Methods
Get Radiology Tree app to read full this article<
Patient Selection
Get Radiology Tree app to read full this article<
CTC Protocol
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
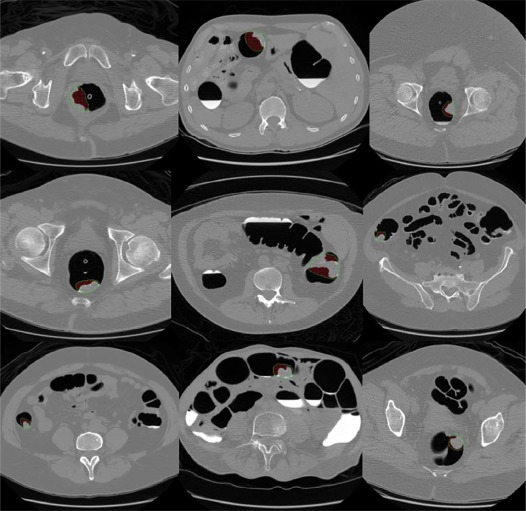
CT Image Reconstruction and Analysis for Human Readers
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
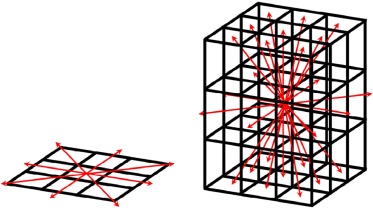
VTA
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Statistical Analysis
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 1
Comparison of Adenocarcinoma and Advanced Adenoma Cohorts
Metric Adenocarcinoma Cohort Advanced Adenoma Cohort_P_ Value All Patients Number of patients 28 31 —– 59 Mean patient age [±SD] (years) 68.9 ± 14.2 64.3 ± 10.3 .157 66.5 ± 12.4 Patient ratio (male : female) 11:17 19:12 .121 40:39 Number of lesions 32 31 —– 63 Mean lesion diameter [±SD] (cm) 4.4 ± 1.3 4.0 ± 1.2 .223 4.2 ± 1.3 Lesion location ratio (right colon : left colon) 15:15 17:16 1.000 32:31
SD, standard deviation.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
TABLE 2
Diagnostic Performance of Human Readers and VTA
Metric Reader 1 Reader 2 Reader 3 All Readers VTA_P_ Value Sensitivity 84.4% 96.9% 93.8% 91.7% 83.6% .034 (27/32) (31/32) (30/32) (88/96) (2675/3200) Specificity 74.2% 77.4% 80.6% 77.4% 87.5% .007 (23/31) (24/31) (25/31) (72/93) (2713/3100) PPV 77.1% 81.6% 83.3% 80.7% 87.4% .057 (27/35) (31/38) (30/36) (88/109) (2675/3062) NPV 82.1% 96.0% 92.6% 90.0% 83.8% .165 (23/28) (24/25) (25/27) (72/80) (2713/3238) Accuracy 79.4% 87.3% 87.3% 84.7% 85.5% .753 (50/63) (55/63) (55/63) (160/189) (5388/6300)
NPV, negative predictive value; PPV, positive predictive value; VTA, volumetric textural analysis.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgments
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Howlader N.N.A., Krapcho M., Miller D., et. al.: SEER Cancer Statistics Review, 1975–2013, National Cancer Institute. Bethesda, MD; Available at https://seer.cancer.gov/archive/csr/1975_2013/ based on November 2015 SEER data submission, posted to the SEER web site; Accessed November 1, 2016
2. Muto T., Bussey H.J.R., Morson B.C.: Evolution of cancer of colon and rectum. Cancer 1975; 36: pp. 2251-2270.
3. Winawer S.J., Zauber A.G., Ho M.N., et. al.: Prevention of colorectal cancer by colonoscopic polypectomy. NEJM 1993; 329: pp. 1977-1981.
4. Bibbins-Domingo K., Grossman D.C., Curry S.J., et. al.: Screening for colorectal cancer: US preventive services task force recommendation statement. JAMA 2016; 315: pp. 2564-2575.
5. Lin J.S., Piper M.A., Perdue L.A., et. al.: Screening for colorectal cancer: updated evidence report and systematic review for the US preventive services task force. JAMA 2016; 315: pp. 2576-2594.
6. Graser A., Stieber P., Nagel D., et. al.: Comparison of CT colonography, colonoscopy, sigmoidoscopy and faecal occult blood tests for the detection of advanced adenoma in an average risk population. Gut 2009; 58: pp. 241-248.
7. Johnson C.D., Chen M.-H., Toledano A.Y., et. al.: Accuracy of CT colonography for detection of large adenomas and cancers. NEJM 2008; 359: pp. 1207-1217.
8. Kim D.H., Pickhardt P.J., Taylor A.J., et. al.: CT colonography versus colonoscopy for the detection of advanced neoplasia. NEJM 2007; 357: pp. 1403-1412.
9. Pickhardt P.J., Choi J.R., Hwang I., et. al.: Computed tomographic virtual colonoscopy to screen for colorectal neoplasia in asymptomatic adults. NEJM 2003; 349: pp. 2191-2200.
10. Hassan C., Zullo A., Laghi A., et. al.: Colon cancer prevention in Italy: cost-effectiveness analysis with CT colonography and endoscopy. Dig Liver Dis 2007; 39: pp. 242-250.
11. Pickhardt P.J., Hassan C., Laghi A., et. al.: Cost-effectiveness of colorectal cancer screening with computed tomography colonography—the impact of not reporting diminutive lesions. Cancer 2007; 109: pp. 2213-2221.
12. Pooler B.D., Kim D.H., Hassan C., et. al.: Variation in diagnostic performance among radiologists at screening CT colonography. Radiology 2013; 268: pp. 127-134.
13. Pickhardt P.J.: CT colonography for population screening: ready for prime time?. Dig Dis Sci 2015; 60: pp. 647-659.
14. Zalis M.E., Barish M.A., Choi J.R., et. al.: CT colonography reporting and data system: a consensus proposal. Radiology 2005; 236: pp. 3-9.
15. Pickhardt P.J., Kim D.H., Pooler B.D., et. al.: Assessment of volumetric growth rates of small colorectal polyps with CT colonography: a longitudinal study of natural history. Lancet Oncol 2013; 14: pp. 711-720.
16. Sievers C.K., Zou L.S., Pickhardt P.J., et. al.: Subclonal diversity arises early even in small colorectal tumours and contributes to differential growth fates. Gut 2017; 66: pp. 2132-2140.
17. Olson T.J.P., Hadac J.N., Sievers C.K., et. al.: Dynamic tumor growth patterns in a novel murine model of colorectal cancer. Cancer Prev Res (Phila) 2014; 7: pp. 105-113.
18. Sottoriva A., Kang H., Ma Z.C., et. al.: A big bang model of human colorectal tumor growth. Nat Genet 2015; 47: pp. 209-216.
19. Song B.W., Zhang G.P., Lu H.B., et. al.: Volumetric texture features from higher-order images for diagnosis of colon lesions via CT colonography. Int J Comput Assist Radiol Surg 2014; 9: pp. 1021-1031.
20. Hu Y.F., Liang Z.R., Song B.W., et. al.: Texture feature extraction and analysis for polyp differentiation via computed tomography colonography. IEEE Trans Med Imaging 2016; 35: pp. 1522-1531.
21. Pickhardt P.J.: Screening CT colonography: how I do it. AJR Am J Roentgenol 2007; 189: pp. 290-298.
22. Borden Z.S., Pickhardt P.J., Kim D.H., et. al.: Bowel preparation for CT colonography: blinded comparison of magnesium citrate and sodium phosphate for catharsis. Radiology 2010; 254: pp. 138-144.
23. Shinners T.J., Pickhardt P.J., Taylor A.J., et. al.: Patient-controlled room air insufflation versus automated carbon dioxide delivery for CT colonography. AJR Am J Roentgenol 2006; 186: pp. 1491-1496.
24. Buchach C.M., Kim D.H., Pickhardt P.J.: Performing an additional decubitus series at CT colonography. Abdom Imaging 2011; 36: pp. 538-544.
25. Horton K.M., Abrams R.A., Fishman E.K.: Spiral CT of colon cancer: imaging features and role in management. Radiographics 2000; 20: pp. 419-430.
26. Iyer R.B., Silverman P.M., DuBrow R.A., et. al.: Imaging in the diagnosis, staging, and follow-up of colorectal cancer. AJR Am J Roentgenol 2002; 179: pp. 3-13.
27. Nerad E., Lahaye M.J., Maas M., et. al.: Diagnostic accuracy of CT for local staging of colon cancer: a systematic review and meta-analysis. AJR Am J Roentgenol 2016; 207: pp. 984-995.
28. Haralick R.M., Shanmugam K., Dinstein I.: Textural features for image classification. IEEE Trans Syst Man Cybern 1973; SMC3: pp. 610-621.
29. Breiman L.: Random forests. Mach Learn 2001; 45: pp. 5-32.
30. Hanley J.A., McNeil B.J.: The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology 1982; 143: pp. 29-36.
31. McNeil B.J., Hanley J.A.: Statistical approaches to the analysis of receiver operating characteristic (ROC) curves. Med Decis Making 1984; 4: pp. 137-150.
32. Sievers C.K., Grady W.M., Halberg R.B., et. al.: New insights into the earliest stages of colorectal tumorigenesis. Expert Rev Gastroenterol Hepatol 2017; in press
33. Yang C.Y., Tseng J.Y., Chen C.F., et. al.: Genome-wide copy number changes and CD133 expression characterized distinct subset of colon polyps: differentiation between incidental polyps and cancer-associated polyps. Int J Colorectal Dis 2015; 30: pp. 1617-1626.