
Rationale and Objectives
Despite its increasing use in training other medical specialties, high-fidelity simulation to prepare diagnostic radiology residents for call remains an underused educational resource. To attempt to characterize the barriers toward adoption of this technology, we conducted a survey of academic radiologists and radiology trainees.
Materials and Methods
An Institutional Review Board-approved survey was distributed to the Association of University Radiologists members via e-mail. Survey results were collected electronically, tabulated, and analyzed.
Results
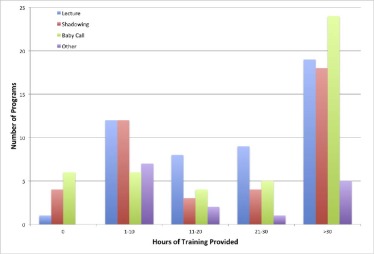
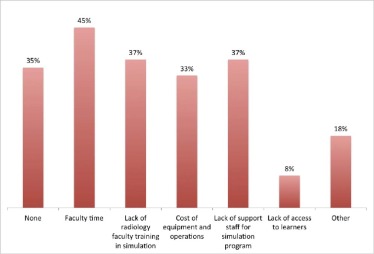
A total of 68 survey responses representing 51 programs were received from program directors, department chairs, chief residents, and program administrators. The most common form of educational activity for resident call preparation was lectures. Faculty supervised “baby call” was also widely reported. Actual simulated call environments were quite rare with only three programs reporting this type of educational activity. Barriers to the use of simulation include lack of faculty time, lack of faculty expertise, and lack of perceived need.
Conclusions
High-fidelity simulation can be used to mimic the high-stress, high-stakes independent call environment that the typical radiology resident encounters during the second year of training, and can provide objective data for program directors to assess the Accreditation Council of Graduate Medical Education milestones. We predict that this technology will begin to supplement traditional diagnostic radiology teaching methods and to improve patient care and safety in the next decade.
Introduction
The use of simulation as a training tool in medicine has grown dramatically in recent years. Between 2000 and 2009, the number of simulation centers in the United States increased from approximately 100 to over 1000 . In particular, this growth in simulation training has also borne out a transition from low-fidelity to high-fidelity simulation (HFS) . HFS is defined as immersing participants into realistic scenarios that mimic real-life encounters. In health care, HFS is implemented using scenarios with tools and techniques and real-time feedback similar or identical to those that would be experienced during actual patient care situations. Medical disciplines such as surgery, anesthesia, obstetrics, emergency medicine, internal medicine, and nursing are using high-fidelity mannequins, sophisticated environments, and virtual reality computer software to simulate disease processes and allow trainees to safely learn and practice complex procedures as well as develop technical skill sets . The impact of HFS training has been demonstrated in the literature. Senior anesthesiology residents were more effective in weaning patients from cardiopulmonary bypass after undergoing an HFS training session rather than an interactive lecture . Nurses and obstetrics residents performed better in managingpatients with shoulder dystocia and eclampsia after dedicated HFS training rather than lectures combined with hands-on demonstrations alone . Furthermore, there are programs conducting fellowships that focus entirely only on training physicians to use simulation medicine as an integral teaching tool .
Within radiology, simulation was recognized over a decade ago as an important technique for teaching procedures in a safe environment . Life-like simulators allow trainees to learn procedures such as guidewire and catheter insertion for vascular interventions . In addition, many residency programs are using simulation environments to give trainees practice in appropriately managing patients who are having adverse reactions to intravenous contrast . A number of researchers have shown that simulation training improves learning and retention of complex skills over more traditional educational methods such as lectures and demonstrations . A cost analysis comparing high-fidelity contrast reaction management training to traditional lecture series demonstrated that the higher cost of developing and implementing the former was offset by the potential high cost of morbidity associated with a mismanaged contrast reaction . A dedicated simulation laboratory course to educate radiology residents on the management of tension pneumothorax, massive hemorrhage, and contrast reactions demonstrated improved post-test scores after the immersion training .
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Materials and Methods
Get Radiology Tree app to read full this article<
Table 1
Survey Questions Distributed to the AUR Membership
Q1 I am a: □ Residency/fellowship program director (1) □ Nonprogram director faculty (2) □ Chief resident (3) □ Other resident/fellow (4) □ Program administrator (5) □ Other (6) ____________________ Q2 Program name/city/state ____________________ Q3 Affiliated medical school ____________________ Q5 Which of the following methods does your program use to prepare residents specifically for independent call? Check all that apply.
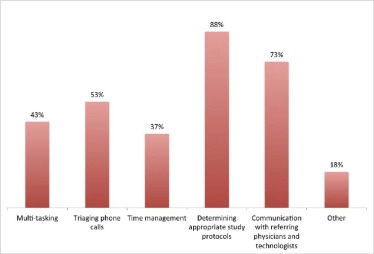
0 hours (1) 1–10 hours (2) 11–20 hours (3) 21–30 hours (4) > 30 hours (5) Lecture (1) □ □ □ □ □ Shadowing Senior Residents (2) □ □ □ □ □ “Baby Call” (limited responsibility with close attending supervision) (3) □ □ □ □ □ Other (please describe) (4) □ □ □ □ □ Q6 Before starting independent call, for which of the following skills do your residents receive specific, focused training? Check all that apply. □ Multi-tasking on call (1) □ Triaging phone calls during the call shift (2) □ Time management on call (3) □ Determining appropriate study protocols (4) □ Communicating with referring physicians and/or technologists during call (5) □ Other (please describe) (6): ____________________ Q8 Before starting independent call, which of the following types of training do your residents receive on how to communicate critical findings? Check all that apply. □ Specific guidelines for what to communicate and how to document the communication (1) □ To whom findings should be communicated (2) □ How the appropriate clinician should be contacted (3) □ No formal training to this effect (4) Q9 What formal training in professional behavior during interactions with clinicians do residents receive before call? ____________________ Q10 What system do you have in place to enable residents to meet the new ACGME milestones? ____________________ Q11 How do you track and/or evaluate residents’ performance during independent call? Who reviews the data? ____________________ Q12 On average, how many hours of training do your residents receive per year on a system that mimics the call environment? □ None (1) □ Not sure (2) □ 1–5 hours (3) □ 6–10 hours (4) □ 11–20 hours (5) □ >21 hours (6) Q13 If you have such a system that mimics the call environment, please describe how it works. ____________________ Q14 What barriers to using a simulated call environment exist within your own department? □ None (1) □ Faculty time (2) □ Lack of radiology faculty training in simulation (3) □ Cost of equipment and operations (4) □ Lack of support staff for center/program (5) □ Lack of access to learners (6) □ Other (please describe) (7) ____________________
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Results
Demographics of Survey Respondents
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Acknowledgment
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Okuda Y., Bond W., Bonfante G., et. al.: National growth in simulation training within emergency medicine residency programs, 2003–2008. Acad Emerg Med 2008; 15: pp. 1113-1116.
2. Sherwin J.: More than make believe: the power and promise of simulation. Biomed Instrum Technol 2012; pp. 254-263.
3. Lewis R., Strachan A., Smith M.M.: Is high fidelity simulation the most effective method for the development of non-technical skills in nursing? A review of the current evidence. Open Nurs J 2012; 6: pp. 82-89.
4. Tan S.C., Marlow N., Field J., et. al.: A randomized crossover trial examining low- versus high-fidelity simulation in basic laparoscopic skills training. Surg Endosc 2012; 26: pp. 3207-3214.
5. Butler K.W., Veltre D.E., Brady D.: Implementation of active learning pedagogy comparing low-fidelity simulation versus high-fidelity simulation in pediatric nursing education. Clin Simul Nurs 2009; 5: pp. e129-e136.
6. Sudikoff S.N., Overly F.L., Shapiro M.J.: High-fidelity medical simulation as a technique to improve pediatric residents’ emergency airway management and teamwork: a pilot study. Pediatr Emerg Care 2009; 25: pp. 651-656.
7. Hunziker S., Bühlmann C., Tschan F., et. al.: Brief leadership instructions improve cardiopulmonary resuscitation in a high-fidelity simulation: a randomized controlled trial. Crit Care Med 2010; 38: pp. 1086-1091.
8. Daniels K., Arafeh J., Clark A., et. al.: Prospective randomized trial of simulation versus didactic teaching for obstetrical emergencies. Simul Healthc 2010; 5: pp. 40-45.
9. Bruppacher H.R., Alam S.K., LeBlanc V.R., et. al.: Simulation-based training improves physicians’ performance in patient care in high-stakes clinical setting of cardiac surgery. Anesthesiology 2010; 112: pp. 985-992.
10. Lo B.M., Devine A.S., Evans D.P., et. al.: Comparison of traditional versus high-fidelity simulation in the retention of ACLS knowledge. Resuscitation 2011; 82: pp. 1440-1443.
11. Tan S.C., Marlow N., Field J., et. al.: A randomized crossover trial examining low-versus high-fidelity simulation in basic laparoscopic skills training. Surg Endosc 2012; 26: pp. 3207-3214.
12. Passiment M., Sacks H., Huang G.: Medical Simulation in Medical Education: Results of an AAMC Survey.2011.
13. Desser T.S.: Simulation-based training: the next revolution in radiology education?. J Am Coll Radiol 2007; 4: pp. 816-824.
14. Anderson J., Chui C.K., Cai Y., et. al.: Virtual reality training in interventional radiology: the Johns Hopkins and Kent Ridge digital laboratory experience. Semin Intervent Radiol 2002; 19: pp. 179-185.
15. Wang F., Duratti L., Samur E., et. al.: A computer-based real-time simulation of interventional radiology. Conf Proc IEEE Eng Med Biol Soc 2007; pp. 1742-1745.
16. Gould D.A.: Interventional radiology simulation: prepare for a virtual revolution in training. J Vasc Interv Radiol 2007; 18: pp. 483-490.
17. Dawson S.: Procedural simulation: a primer. J Vasc Interv Radiol 2006; 17: pp. 205-213.
18. Tofil N.M., White M.L., Grant M., et. al.: Severe contrast reaction emergencies. High-fidelity simulation training for radiology residents and technologists in a children’s hospital. Acad Radiol 2010; 17: pp. 934-940.
19. Wang C.L., Schopp J.G., Kani K., et. al.: Prospective randomized study of contrast reaction management curricula: computer-based interactive simulation versus high-fidelity hands-on simulation. Eur J Radiol 2013; 82: pp. 2247-2252.
20. Wang C.L., Schopp J.G., Petscavage J.M., et. al.: Prospective randomized comparison of standard didactic lecture versus high-fidelity simulation for radiology resident contrast reaction management training. AJR Am J Roentgenol 2011; 196: pp. 1288-1295.
21. Tubbs R.J., Murphy B., Mainiero M.B., et. al.: High-fidelity medical simulation as an assessment tool for radiology residents’ acute contrast reaction management skills. J Am Coll Radiol 2009; 6: pp. 582-587.
22. Petscavage J.M., Wang C.L., Schopp J.G., et. al.: Cost analysis and feasibility of high-fidelity simulation based radiology contrast reaction curriculum. Acad Radiol 2011; 18: pp. 107-112.
23. Sarwani N., Tappouni R., Flemming D.: Use of a simulation laboratory to train radiology residents in the management of acute radiologic emergencies. AJR Am J Roentgenol 2012; 199: pp. 244-251.
24. Niell B.L., Kattapuram T., Halpern E.F., et. al.: Prospective analysis of an interprofessional team training program using high-fidelity simulation of contrast reactions. AJR Am J Roentgenol 2015; 204: pp. W670-W676.
25. Sabir S.H., Aran S., Abujudeh H.: Simulation-based training in radiology. J Am Coll Radiol 2014; 11: pp. 512-517. Elsevier
26. Picard M., Curry N., Collins H., et. al.: Comparison of high-fidelity simulation versus didactic instruction as a reinforcement intervention in a comprehensive curriculum for radiology trainees in learning contrast reaction management: does it matter how we refresh?. Acad Radiol 2015; 22: pp. 1268-1276.
27. Ahmad R., Alhashmi G., Ajlan A., et. al.: Impact of high-fidelity transvaginal ultrasound simulation for radiology on residents’ performance and satisfaction. Acad Radiol 2015; 22: pp. 234-239.
28. Ganguli S., Camacho M., Yam C.S., et. al.: Preparing first-year radiology residents and assessing their readiness for on-call responsibilities: results over 5 years. AJR Am J Roentgenol 2009; 192: pp. 539-544.
29. Towbin A.J., Paterson B., Chang P.J.: A computer-based radiology simulator as a learning tool to help prepare first-year residents for being on call. Acad Radiol 2007; 14: pp. 1271-1283.
30. Towbin A.J., Paterson B.E., Chang P.J.: Computer-based simulator for radiology: an educational tool. Radiographics 2008; 28: pp. 309-316.
31. Ganguli S., Pedrosa I., Yam C.-S., et. al.: Part I: preparing first-year radiology residents and assessing their readiness for on-call responsibilities. Acad Radiol 2006; 13: pp. 764-769.
32. Yam C.S., Kruskal J., Pedrosa I., et. al.: Preparing and assessing first-year radiology resident on-call readiness. Technical implementation. Acad Radiol 2006; 13: pp. 770-773.
33. Soman S., Amorosa J.K., Mueller L., et. al.: Evaluation of medical student experience using medical student created student PACS flash based PACS simulator tutorials for learning radiological topics. Acad Radiol 2010; 17: pp. 799-807.
34. Balint B.J., Steenburg S.D., Lin H., et. al.: Do telephone call interruptions have an impact on radiology resident diagnostic accuracy?. Acad Radiol 2014; 21: pp. 1623-1628. Elsevier Ltd
35. Accreditation Council for Graduate Medical Education : ACGME Common Program Requirements.2015.
36. Education AC for GM, American Board of Radiology : The Diagnostic Radiology Milestone Project.2015.
37. National Residency Matching Program : Results and Data: 2015 Main Residency Match.2015.