
Rationale and Objectives
Patient-centered care has become a primary focus in clinical practice. In developing practice guidelines for clinical care, the patients’ perspective is an important component.
Materials and Methods
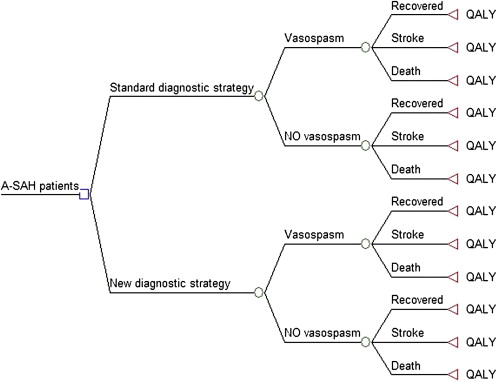
Patients’ preferences are represented in a decision analytic model as quality-of-life weights for different health states associated with the aneurysmal subarachnoid hemorrhage population. The time–tradeoff method is used to obtain the individual patients’ preferences, which are directly measured in quality-adjusted life years. An individualized care model is explained as a means of implementing a patient-centered approach into practice guidelines for clinical care. A method for calculating the expected value for societal benefit from improved decision making using an individualized care model is reviewed.
Results
We discuss our work-in-progress towards incorporating patients’ preferences in a decision analytic model for aneurysmal subarachnoid hemorrhage patients. The main methodologic concerns for using patients’ preferences in cost-effectiveness analyses for developing practice guidelines are discussed.
Conclusion
Emphasis is placed on using patients’ preferences and patient-centered outcome measures in cost-effectiveness analyses.
In recent years, there has been improved awareness and effort to implement patient-centered care in clinical practice. With the advent of patient involvement in addressing health care issues and government policy making, patient-centered care has become a primary focus in developing practice guidelines. In this setting, the patient is considered as the ultimate judge of the quality of medical care services. By applying this concept specifically to radiology practice, the patient is regarded as the authority on determining an imaging experience as acceptable care, including the outcome management from the examination performed. Thereby, patients’ preferences and patient-centered outcomes are an important component in developing practice guidelines for clinical care.
Practice guidelines have been defined as systematically developed statements to assist both physicians and patients in making decisions about appropriate health care for specific clinical circumstances . Issues related to costs, benefit, quality, access, patients’ preferences, and utilization are some factors considered in developing practice guidelines. Emphasis is placed on developing systematic practice guidelines using evidence-based medicine, such as conclusions drawn from decision analyses to determine quality of life and cost-effectiveness.
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Decision analytic model
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Incorporating Patients’ Preferences
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Measuring The Expected Value Of Individualized Care
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. Institute of Medicine 1990 Report: Clinical Practice Guidelines: Directions for a New Program.
2. Basu A., Meltzer D.: Value of information on preference heterogeneity and individualized care. Med Decis Making 2007; 27: pp. 112-127.
3. Wartenberg K.E., Schmidt J.M., Claassen J., et. al.: Impact of medical complications on outcome after subarachnoid hemorrhage. Crit Care Med 2006; 34: pp. 617-623.
4. Mori K., Arai H., Nakajima K., et. al.: Hemorheological and hemodynamic analysis of hypervolemic hemodilution therapy for cerebral vasospasm after aneurysmal subarachnoid hemorrhage. Stroke 1995; 26: pp. 1620-1626.
5. Dorsch N.W.: The effect and management of delayed vasospasm after aneurysmal subarachnoid hemorrhage. Neurol Med Chir 1998; 38: pp. S156-S160.
6. Kallmes D.F., Kallmes M.H., Cloft H.J., et. al.: Guglielmi detachable coil embolization for unruptured aneurysms in nonsurgical candidates: a cost-effectiveness exploration. AJNR Am J Neuroradiol 1998; 19: pp. 167-176.
7. Yoshimoto Y., Wakai S.: Cost-effectiveness analysis of screening for asymptomatic, unruptured intracranial aneurysms. A mathematical model. Stroke 1999; 30: pp. 1621-1627.
8. Kallmes D.F., Kallmes M.H.: Cost-effectiveness of angiography performed during surgery for ruptured intracranial aneurysms. AJNR Am J Neuroradiol 1997; 18: pp. 1453-1462.
9. Hunink M., Glasziou P.: Valuing outcomes.Hunink M.Glasziou P.Decision making in health and medicine.2001.Cambridge University PressUnited kingdom: 103–105
10. Torrance G.W., Thomas W.H., Sackett D.L.: A utility maximization model for evaluation of health care programs. Health Serv Res 1972; 7: pp. 118-133.
11. Sommers B.D., Beard C.J., D’Amico A.V., et. al.: Decision analysis using individual patient preferences to determine optimal treatment for localized prostate cancer. Cancer 2007; 110: pp. 2210-2217.
12. Albertsen P.C., Nease R.F., Potosky A.L.: Assessment of patient preferences among men with prostate cancer. J Urol 1998; 159: pp. 158-163.
13. Wennberg J.E.: On patient need, equity, suppler induced demand, and the need to assess the outcome of common medical practices. Med Care 1985; 23: pp. 512-520.
14. Fryback D.F., Dasbach E.J., Klein R., et. al.: The Beaver Dam Health Outcomes Study: initial catalog of health-state quality functions. Med Decis Making 1993; 13: pp. 89-102.
15. Kim D.H., Haney C.L., Ginhoven G.V.: Utility of outcome measures after treatment for intracranial aneurysms. Stroke 2005; 36: pp. 792-796.
16. King J.T., Kassam A.B., Yonas H., et. al.: Mental health, anxiety, and depression in patients with cerebral aneurysms. J Neurosurg 2005; 103: pp. 636-641.
17. Toomela A., Pulver A., Tomberg T., et. al.: Possible interpretation of subjective complaints in patients with spontaneous subarachnoid hemorrhage. J Rehabil Med 2004; 36: pp. 63-69.
18. King J.T., Horowitz M.B., Kassam A.B., et. al.: The short form-12 and the measurement of health status in patients with cerebral aneurysms: performance, validity, and reliability. J Neurosurg 2005; 102: pp. 489-494.
19. Meltzer D, Huang ES, Brown SES, et al. Effects of patient self-selection on cost-effectiveness: implications for intensive therapy for diabetes. Poster presentation at the 27th annual meeting of the Society for Medical Decision Making. October 21-24, 2005; San Francisco.
20. Swan J.S., Fryback D.G., Lawrence W.F., et. al.: A time-tradeoff method for cost-effectiveness models applied to radiology. Med Decis Making 2000; 20: pp. 79-88.
21. Hunink M., Glasziou P.: Constrained resources.Hunink M.Glasziou P.Decision making in health and medicine.2001.Cambridge University PressUnited Kingdom: 268–269