
Rationale and Objectives
Single brain malignancy (SBM) often poses a diagnostic dilemma, with differential diagnosis of primary brain malignancy (PBM) versus metastasis commonly rendered. This study assesses the yield of preoperative computed tomography (CT) of the chest, abdomen, and pelvis (CTCAP) in patients with SBM.
Materials and Methods
Institutional review board (IRB)-approved retrospective review of the imaging database at a tertiary-care center was performed for patients with magnetic resonance findings compatible with a diagnosis of SBM. Demographic information, lesion characteristics (location and size), and pathology were recorded. Findings of CTCAP for metastatic workup prior to SBM excisional biopsy were also documented, if performed.
Results
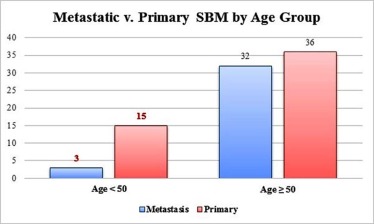
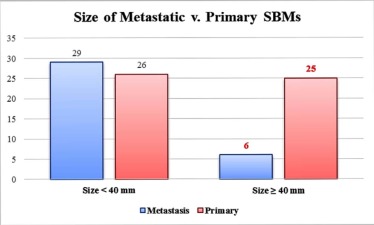
Eighty-six of 92 patients with new diagnosis of SBM on MR imaging had subsequent lesion resection and pathology consistent with malignancy. PBM accounted for 51 cases (59%) and metastasis accounted for 35 cases (41%). When stratified by age group, PBM was more common in patients <50 years old (15 of 18 (83%)), whereas similar rates of PBM and metastatic disease were identified in older patients. When stratified by lesion size, PBM was more common in tumors ≥40 mm (25 of 31 (81%)), whereas similar rates of PBM and metastatic disease were identified in smaller lesions. Lung cancer was the most common CTCAP and pathology-confirmed source of metastatic SBM (68% and 66%, respectively).
Conclusions
The yield of preoperative CTCAP can be increased by targeting patients older than 50 years of age with SBMs smaller than 40 mm in size.
Introduction
Primary brain malignancy is relatively common, with an expected incidence of 25,000 cases in 2016 according to the Central Brain Tumor Registry of the United States . Brain metastases are even more common than primary brain malignancy, with an estimated yearly incidence of 40,000 cases . Contrast-enhanced magnetic resonance imaging (MRI) is the imaging test of choice for detecting and characterizing brain tumors, and a normal contrast-enhanced MRI essentially rules out malignancy. Multiple ring enhancing neoplasms in the brain are usually metastases and do not cause a diagnostic dilemma. However, single enhancing neoplasms often pose a challenge as both primary intra-axial tumor and solitary metastasis may have a similar appearance. This becomes even more problematic given the similar rates of primary and metastatic malignancies in the setting of single brain malignancies (SBMs), specifically . Further adding to the confusion, approximately half of all brain metastases are single , and about 70% of all patients with brain metastases have three or fewer lesions at the time of detection . Several findings at routine magnetic resonance (MR) imaging have been described to attempt to distinguish between the two entities , but commonly a differential diagnosis of primary brain malignancy versus metastasis is still rendered, precipitating our clinical colleagues to pursue computed tomography (CT) of the chest, abdomen, and pelvis (CTCAP) prior to SBM excisional biopsy in search of a potential extracranial primary malignancy. Our goal is to characterize the yield of preoperative CTCAP in patients with SBM diagnosed on imaging.
Methods
Subjects
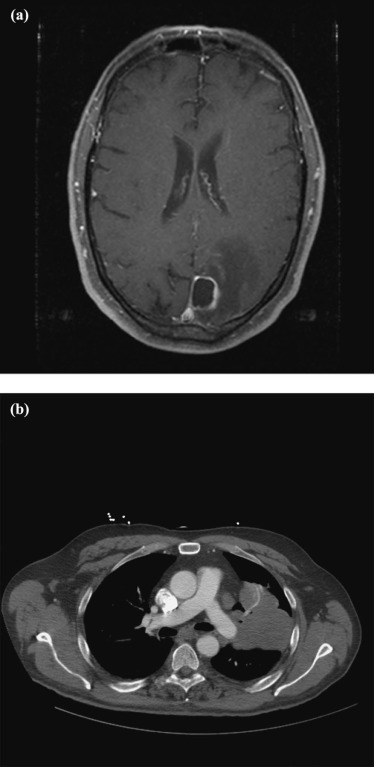
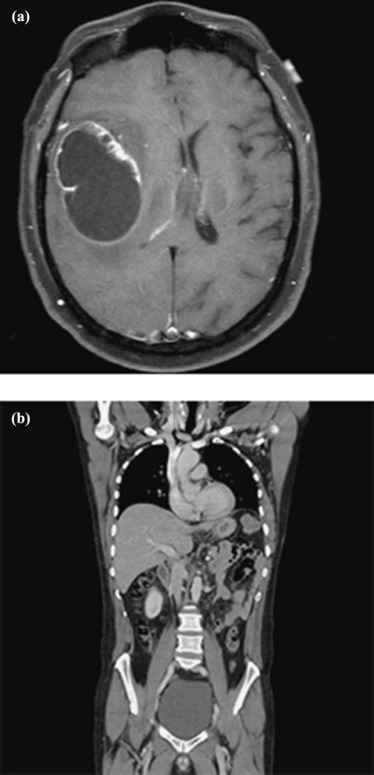
Following IRB approval, a retrospective review of an imaging database at a tertiary-care center was performed for patients with a new diagnosis of a single brain lesion suspicious for malignancy found on brain imaging. The time period of data collection was from 2008 to 2013. The search terms used were “single, solitary, brain, malignancy, metastasis, primary.” Only positive cases were reviewed. The search engine used was Primordial (Primordial Inc, San Mateo, CA). MR imaging of the brain was the imaging modality used to assess for SBM due to its ability to detect small lesions: additional lesions can be occult on enhanced and unenhanced CT. MR also provides increased specificity for diagnosis of brain malignancy, by distinguishing between other potential etiologies, such as brain abscesses (which typically show restricted diffusion centrally, arguing against malignancy) . Only patients with single brain neoplasms who had a subsequent lesion resection confirming malignancy (primary or metastatic) were included in this study. Patient demographic information (sex, age), lesion MR characteristics (location, size, signal characteristics), and pathology results were recorded. Findings of CTCAP for preoperative metastatic workup were also documented, if performed. The majority of the CTCAPs were performed within 24 hours, and all were performed within 3 days (before SBM excisional biopsy was attempted). Exemplar brain MR and body CT imaging are provided in Figures 1 and 2 .
Get Radiology Tree app to read full this article<
Statistics
Get Radiology Tree app to read full this article<
Results
Get Radiology Tree app to read full this article<
SBM Pathology
Get Radiology Tree app to read full this article<
Patient Age
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
SBM Size
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
SBM Size Stratified by Patient Age
Get Radiology Tree app to read full this article<
CTCAP
Get Radiology Tree app to read full this article<
TABLE 1
Characteristics of CTCAP Versus Non-CTCAP Group in 86 Patients Who Underwent Resection
CTCAP Non-CTCAP Total number 58 28 Average age (range) 64 years (30–86) 52 years (19–89) Male (%) 34/58 (59%) 13/28 (46%) Female (%) 22/58 (41%) 15/28 (54%) Average tumor size (range) 36 mm (12–78 mm) 43 mm (13–80 mm) Primary brain malignancy (%) 26/58 (45%) 25/28 (89%) Metastasis (%) 32/58 (55%) 3/28 (11%)
CTCAP, computed tomography of the chest, abdomen, and pelvis.
Get Radiology Tree app to read full this article<
Discussion
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
Conclusion
Get Radiology Tree app to read full this article<
Acknowledgment
Get Radiology Tree app to read full this article<
Get Radiology Tree app to read full this article<
References
1. CBTRUS : 2015 Central Brain Tumor Registry of the United States fact sheet. Available at: http://www.cbtrus.org/factsheet/factsheet.html Accessed November 23, 2015
2. Gavrilovic I., Posner J.: Brain metastases: epidemiology and pathophysiology. J Neuro-Oncol 2005; 75: pp. 5-14.
3. Voorhies R.M., Sundaresan N., Thaler H.T.: The single supratentorial lesion: an evaluation of preoperative diagnostic tests. J Neurosurg 1980; 53: pp. 364-368.
4. Schwartz K., Erikson B., Luccinetti C.: Pattern of T2 hypointensity associated with ring-enhancing lesions can help to differentiate pathology. Neuroradiology 2006; 48: pp. 143-149.
5. Nussbaum E., Djalilian H., Cho K., et. al.: Brain metastases. Histology, multiplicity, surgery, and survival. Cancer 1996; 78: pp. 1781-1788.
6. Delattre J., Krol G., Thaler H., et. al.: Distribution of brain metastases. Arch Neurol 1988; 45: pp. 741-744.
7. Chen X., Yin M., Ai L., et. al.: Differentiation between brain glioblastoma multiforme and solitary metastasis: qualitative and quantitative imaging based on routine MR imaging. Am J Neuroradiol 2012; 33: pp. 1907-1912.
8. Tang Y., Ngai S., Stuckey S.: The solitary enhancing cerebral lesion: can FLAIR aid the differentiation between glioma and metastasis?. Am J Neuroradiol 2006; 27: pp. 609-611.
9. Wang S., Kim S., Poptani J., et. al.: Diagnostic utility of diffusion tensor imaging in differentiating glioblastomas from brain metastases. Am J Neuroradiol 2014; 35: pp. 928-934.
10. Cha S., Lupo J., Lamborn K., et. al.: Differentiation of glioblastoma multiforme and single brain metastasis by peak height and percentage of signal intensity recovery derived from dynamic susceptibility-weighted contrast-enhanced perfusion MR imaging. Am J Neuroradiol 2007; 28: pp. 1078-1084.
11. Bulakbasi N., Kocaoglu M., Farzaliyev A., et. al.: Assessment of diagnostic accuracy of perfusion MR imaging in primary and metastatic solitary brain tumors. Am J Neuroradiol 2005; 26: pp. 2187-2199.
12. Lai P., Ho J., Chen W., et. al.: Brain abscess and necrotic tumor: discrimination with proton MR spectroscopy and diffusion-weighted imaging. Am J Neuroradiol 2002; 23: pp. 1369-1377.
13. Chan S., Lai P., Chen W., et. al.: Diffusion-weighted MRI features of brain abscess and cystic or necrotic brain tumors: comparison with conventional MRI. Clin Imaging 2002; 26: pp. 227-236.
14. Barnholtz-Sloan J.S., Sloan A.E., Davis F.G., et. al.: Incidence proportions of brain metastases in patients diagnosed (1973 to 2001) in the Metropolitan Detroit Cancer Surveillance System. J Clin Oncol 2004; 22: pp. 2865-2872.
15. Schouten L.J., Rutten J., Huveneers H.A.M., et. al.: Incidence of brain metastases in a cohort of patients with carcinoma of the breast, colon, kidney, and lung and melanoma. Cancer 2002; 94: pp. 2698-2705.
16. LeFranc F., Sadeghi N., Camby I., et. al.: Present and potential future issues in glioblastoma treatment. Expert Rev Anticancer Ther 2006; 6: pp. 719-732.
17. Lassman A., DeAngelis L.: Brain metastases. Neurol Clin N Am 2003; 21: pp. 1-23.
18. Patchell R.A., Tibbs P.A., Walsh J.W., et. al.: A randomized trial of surgery in the treatment of single metastases to the brain. N Engl J Med 1990; 322: pp. 494-500.
19. Park S.H., Audu P.B., Sperling M.R., et. al.: Reevaluation of surgery for the treatment of brain metastases: review of 208 patients with single or multiple brain metastases treated at one institution with modern neurosurgical techniques. Neurosurgery 2005; 56: pp. 1021-1034.
20. ACR : Updated 2014 Medicare physician fee schedule payment impact tables for radiology and radiation oncology services. Am Coll Radiol 2014; Available at: http://www.acr.org/News-Publications/News/News-Articles/2013/Economics/20131213-2014-Medicare-Physician-Fee-Schedule-Payment-Cuts Accessed January 6, 2015
21. Siddiqui A.: The multiple procedure payment reduction. Soc Imaging Inform Med 2014; Available at: http://www.siim.org/?page=multiple_procedure_p Accessed January 6, 2015
22. ACR : ACR–AAPM practice parameter for diagnostic reference levels and achievable doses in medical X-ray imaging. Am Coll Radiol 2014; Available at: http://www.acr.org/~/media/ACR/Documents/PGTS/guidelines/Reference_Level%20s_Diagnostic_Xray.pdf Accessed January 6, 2015